
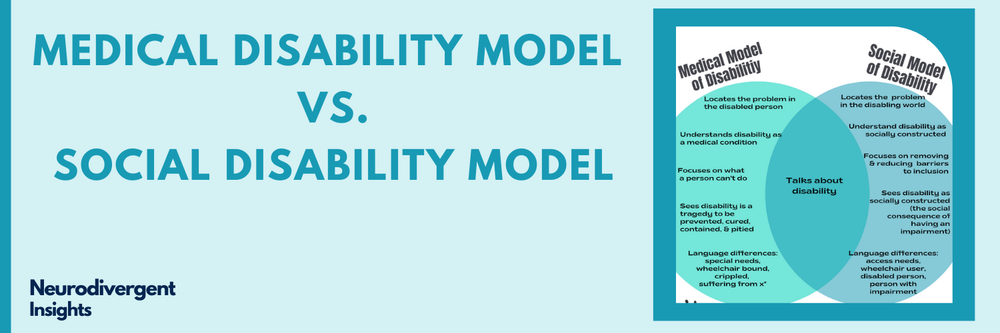
Medical vs Social Models of Disabilities
I have been trained to eat, breathe, and work within the traditional “medical model” of disabilities. And so, when I first learned about the social disability model, it took a bit for my mind to adjust! I have come to deeply appreciate it, particularly in my work with neurodivergent people (and as a neurodivergent person!). Within the medical model, disability is typically defined as something a person lacks, while within the social disability model, it is defined as an experience a person with physical or mental limitations has within an unfair social system. Lisicki summaries this paradigm well:
“The Social Model frames disability as something that is socially constructed. Disability is created by physical, organizational and attitudinal barriers and these can be changed and eliminated. This gives us a dynamic and positive model that tells us what the problem is and how to fix it. It takes us away from the position of “blaming” the individual for their shortcoming. It states that impairment is, and always will be, present in every known society, and therefore the only logical position to take, is to plan and organize society in a way that includes, rather than excludes, Disabled people.”
───Barbara Lisicki, 2013 (source)
History of the Social Disability Model
Inspired by the Civil rights movements in the 1960’s and 1970s, disabled people began connecting, thinking, and talking about their experiences of being excluded, discriminated, and institutionalized. They began thinking critically about the institutional practices and prejudices that perpetuated these dynamics and about how society would need to change for disabled people to have the same rights and opportunities. Thus the “Disability People’s Rights Movement” was born. Several organizations emerged that began thinking about disability through a civil rights and equality lens. This emergent framework became known as the social disability model. It has continued to evolve and expand over the last 40 years.
The social disability model was developed in direct opposition to the dominant medical model and charity model of disability. The traditional paradigm emphasized disability as an individual and medical issue. Issues that needed to be prevented, cured, and contained.
“The Social Model of Disability, developed over the last 40 years by Disabled people, is a radically different Model to the Medical and Charitable approach to disability described above. It states that people have impairments but that the oppression, exclusion, and discrimination people with impairments face is not an inevitable consequence of having an impairment, but is caused instead by the way society is run and organised.” (Source: Inclusion London Fact Sheet)
Understanding the Societal Barriers that Disable People
While traditional medical and charity models focus on what a person cannot do, the social disability model identifies key disabling barriers that “disable” the person.
“Barriers “disable” by creating exclusion, discrimination and disadvantage for people with impairments.” (Source: Inclusion London: The Social Disability Model FactSheets)
The social disability model provides a sort of “roadmap” for identifying and then removing, reducing, or accommodating for these societal barriers. The societal barriers can be categorized as: 1) Attitudinal barriers, physical barriers, and information/communication barriers.
Attitudinal barriers
Attitudinal barriers consist of “social and cultural attitudes and assumptions about people with impairments that explain, justify, and perpetuate prejudice, discrimination, and exclusion in society. For example, assumptions that people with certain impairments can’t work, can’t be independent, can’t have sex, shouldn’t have children, need protecting, are “child-like”, are “dangerous”, should not be seen (because they are upsetting), are scroungers, etc.” (Source: Inclusion London Fact Sheet)
Physical barriers
Physical barriers and barriers that are “linked to the physical and built environment, and cover a huge range of barriers that prevent equal access, such as stairs/ steps, narrow corridors and doorways, curbs, inaccessible toilets, inaccessible housing, poor lighting, poor seating, broken lifts, or poorly managed street and public spaces.” (Source: Inclusion London Fact Sheet)
Information/Communication Barriers
Communication and information barriers include barriers to accessing information and communication. Such as access to interpreters for Deaf people, and lack of information in different accessible formats.
Impairment vs disability
While traditional models of disability tend to locate it within the person, social disability models locate it within the disabling society. When I first learned about the social disability model, I was concerned that this model may minimize people’s experience of suffering and struggle. However, what helped me wrap my mind around this was when I learned about the difference between impairment vs. disability. The social disability model does not refute or minimize the reality of impairment that is present. However, it does distinguish between impairment and disability. Impairment is understood as a person’s “physical, sensory, or cognitive difference” (for example, being blind or deaf, experiencing bipolar, having M.S., being autistic or ADHD, or having a limb difference). This is juxtaposed with Disability which is the “name for the social consequences of having an impairment. People with impairments are disabled by society, so disability is therefore a social construct that can be changed and removed” (Inclusion London Fact Sheet). Once I understood the difference between impairment and disability, I was able to understand how the social disability model socially constructs disability without minimizing or negative the organic impairment that is present for the disabled person.
Use of Language
Another key difference between the medical model and social disability model is the use of language. While the medical model (and charity model to some degree) tends to focus on “negative, charitable and medical views of disability” such as “handicapped”, “cripple”, “wheelchair bound”, “retarded”, “suffering from” and “special needs,” the social model rejects such negative and pathologizing language and replaces it with descriptive language (Inclusion London Fact Sheet). For example, “Disabled person” (not “handicapped” or “cripple”), “wheelchair user” (not “wheelchair bound”), “person with learning difficulties” (not “retarded”), “person with an impairment” (not “suffering from”) and “access needs” (not “special needs”) (Inclusion London Fact Sheet).
In my Psychology training, I learned to always use “person-first language” (for example, a “person with a disability” NOT “disabled person”. The aim of this is to distance from the disability and center the person. This line of thinking makes sense if a) we are locating disability within the person and b) we are assigning value to being disabled. However, the social model of disability has such a different framework that these premises break down. From the framework of the social disability model, the term “disabled people” or “disabled person” is not a bad word. There is no value judgment on that person, rather it is a social-political descriptor of what the person is experiencing. It captures that the person experiences a “disabling experience that people with impairments face in society. It is used to bring together a very diverse group of people with impairments to identify the causes of our discrimination and oppression, communicate shared experience and knowledge, and create social change” (Inclusion London Fact Sheet).
One of the critiques of identity-first language “person with disabilities” is that it is conflating impairment with disability. it is implying that disability is individual vs. social, it is a thing a person has, vs an experience that arises from a person’s interaction with a disabling society. Rather than the person “having a disability, it is the disabling barriers operating in society that disables us—not our impairments” (Inclusion London Fact Sheet).
Pillars of Independent Living
The Social Model of Disability is “dynamic and effective in that it focuses on barriers and solutions to such barriers and, in doing so, maps out an approach to inclusion and equality that is of benefit to society as a whole, not just Disabled people.” Inclusion London: The Social Disability Model FactSheets). The model emphasizes “Pillars of Independent Living”. These pillars are outlined as the following:
Pillars of independent living (Source: Inclusion London: The Social Disability Model FactSheets)
Appropriate and accessible information
An adequate income
Appropriate and accessible health and social care provision
A fully accessible transport system
Full access to the environment
Adequate provision of technical aids and equipment
Availability of accessible and adapted housing
Adequate provision of personal assistance
Availability of inclusive education and training
Equal opportunities for employment
Availability of independent advocacy and self-advocacy
Availability of peer counseling
Conclusion and Critique
The social disability model has faced critique by some disabled people, largely associated with it’s failures in addressing specific experiences and needs of different groups. It also has faced criticism from those experiences chronic medical conditions. The theory is still growing and expanding. As someone trained within the Psychology paradigm, this is a new framework for me. I would love to hear from others who are in the medical field and working to integrate the medical models we work in with the social disability model.
This post was proofread by Grammarly, my go-to for proofreading and catching all the details I naturally miss! Grammarly is entirely free to use. Click here to give it a try.
Featured






")
