
ADHD vs. ODD
I have been hesitant to create this Venn diagram as part of my #ADHD misdiagnosis series. I have been hesitant because I don’t particularly like the diagnosis of ODD. However, I didn’t want to let my bias influence my process, and the reality is that up to 40% of ADHD children are also diagnosed with ODD (Miller), so it felt like an important topic to speak to.
What is Wrong with the ODD Diagnosis?
As I dove into the research, the more problematic the ODD diagnosis felt to me. I won’t make this article a stump speech on ODD, but I want to highlight my concerns with the diagnosis itself.
It is a behavioral disorder, meaning it captures the child’s pattern of behavior but fails to capture the “why” behind the behavior. It is often used as a catch-all diagnosis that captures a kid’s behavior but misses the underlying reason for the behavior. For example, defiant and angry outbursts are common among depressed children, especially boys. It’s also common among anxious children; it can also be a response to trauma or race-based discrimination. It can be sensory-driven and related to underlying neurological differences (i.e., ADHD and autism). My fear is that the diagnosis of ODD stops curiosity, and the kid’s behavior becomes the focus of treatment. To really support these children, we need to understand what is happening beneath the surface that makes this behavior make sense.
Emerging research suggests ODD is likely overly diagnosed in Black and non-white Hispanic children, particularly Black boys (Ballentine, 2019). A white child with a similar presentation is more likely to be diagnosed with an adjustment disorder or with ADHD. A diagnosis of ODD in a Black or brown child can set them down a systemic trajectory that leads to devasting consequences. The overdiagnosis also perpetuates harmful stereotypes about Black boys and Black men (To learn more about ADHD, ODD and racial bias see my infographic about it here).
With that said, there may be some cases where the diagnosis may open up necessary supports such as: parenting training/support and additional emotional-regulation resources. Some families may find it helpful to have a name for the pattern of behavior they are working with. While I would be extremely cautious diagnosing this myself and particularly cautious before diagnosing a BIPOC child with ODD, I am also hesitant to make umbrella statements. There may be situations where such a diagnosis can be useful.
ODD Overview
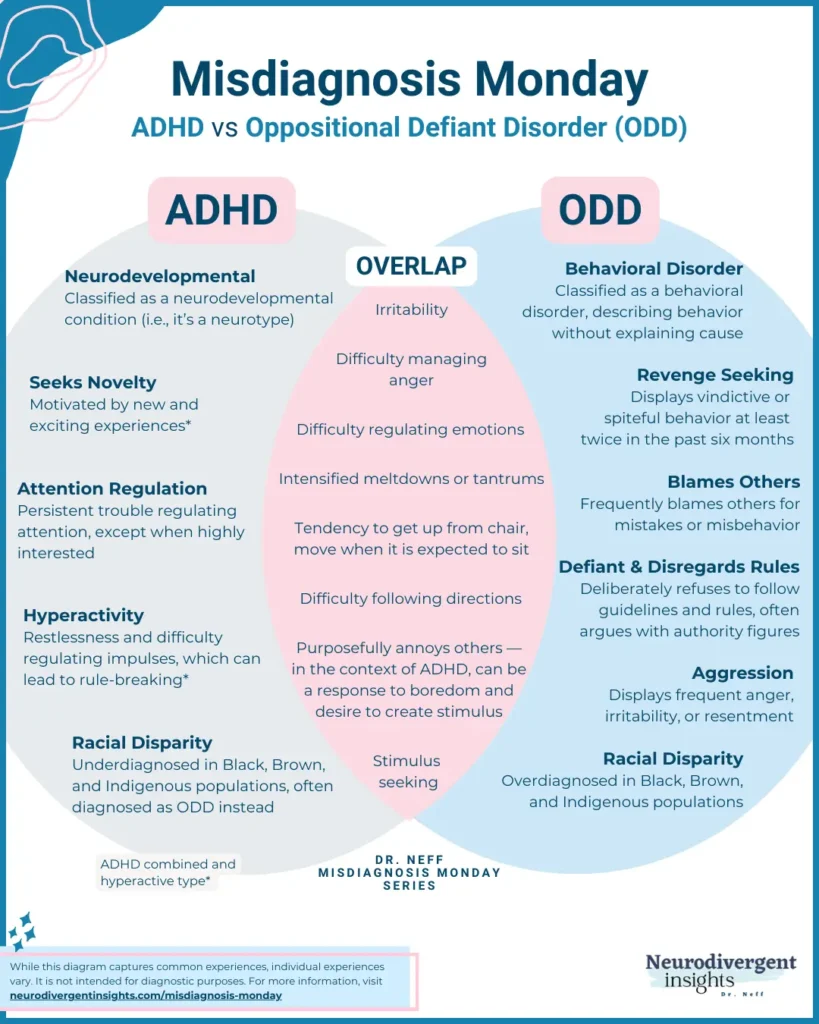
While ADHD is a neurodevelopmental condition, ODD is classified as a disruptive behavioral disorder. The two major disruptive behavior disorders include Oppositional Defiant Disorder and Conduct disorder (CD). Both capture a clustering of behavioral patterns. Children diagnosed with ODD are often described as “uncooperative, defiant, and hostile toward peers, parents, teachers, and other authority figures” (Hopkins Medicine). While ODD is often diagnosed among younger children, CD is often not diagnosed until the teenage years. Both of these behavioral disorders co-occur with ADHD at a high frequency. Fadus et al., 2020 provide a helpful summary of these two diagnoses and their distinctions:
“ODD is characterized by a pervasive pattern of angry and irritable mood, argumentative tendencies, defiant behavior, and vindictiveness. Children and adolescents with ODD frequently lose their temper, are easily annoyed with others, and will often argue with authority figures or refuse to comply with rules. A diagnosis of CD is assigned when behaviors violate the rights of others and major societal norms, including bullying, threatening others, initiating physical fights, sexual assault, and stealing. Although ODD is often thought of as a precursor diagnosis to CD, many children who receive a diagnosis of ODD do not go on to subsequently develop CD”
How is ODD Diagnosed?
For a child to meet the diagnostic criteria for ODD, 4 of the following behaviors must be present for at least the last six months.
Often loses temper
Is often touchy or easily annoyed
Is often angry and resentful
Often argues with authority figures or, for children and adolescents, with adults
Often actively defies or refuses to comply with requests from authority figures or with rules
Often deliberately annoys others
Often blames others for their mistakes or misbehavior
Has been spiteful or vindictive at least twice in the past six months
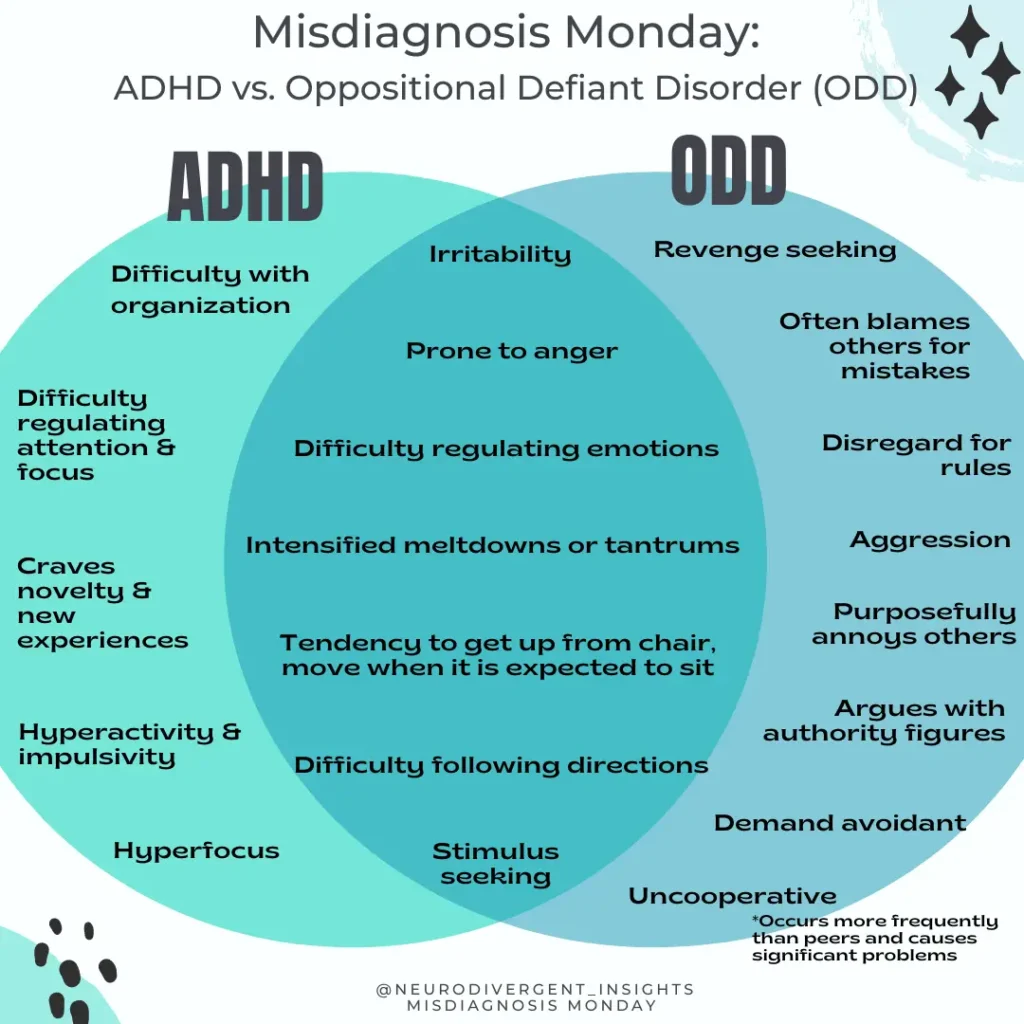
All children experience temper tantrums, can be irritable, or refuse to comply with directions. And so, to meet the criteria, the child must be displaying these behaviors more frequently (and with more intensity) than their peers, and it must create significant problems. ODD Is more common when a child has experienced adverse childhood experiences and more common when they’ve been exposed to certain parenting styles. Therefore one component of ODD treatment often involves parenting support and training.
While the diagnoses of ADHD and ODD co-occur often, there are several reasons that an ADHD child may present with ODD. When these conditions co-occur, it is essential to stay curious and consider the underlying why behind the behavior.
Overlapping ADHD-ODD Traits
Difficulty Controlling Impulsive Behavior
ADHD is characterized by difficulty with top-down executive functioning processes, resulting in disinhibition and impulsivity. Difficulty with impulsivity may lead to behaviors that are classified under ODD.
Hyperactivity
ADHD-H children are more likely to be diagnosed with co-occurring ODD. With hyperactivity, the body needs to move and needs stimulus. Suppose a child is expected to sit still for prolonged periods. In that case, this may lead to disruption and “defiance” as they get up to leave their chair, or alternatively, they may become more agitated and irritable as their bodies aren’t able to regulate through movement. The excessive need for movement thus may lead to some of the more disruptive behaviors that fit the ODD profile.
Stimulus Seeking
In the context of ADHD, it can feel intolerable when there is not enough stimulus. And the ADHD brain is drawn to the new, shiny thing. This may mean a child darts off to go check something new and exciting out, it also can mean if there isn’t enough stimulus, the child will pick a fight with a sibling or peer to create stimulus. This may present as a tendency to bother others.
Sensory Based
Sensory sensitives can lead to increased irritability and reactivity. A child may say no to demands or requests because they are so overloaded and just coping with their sensory environment. Requests to task-switch or do something else are experienced as another sensory request increasing the child’s already overwhelmed sensory system.
Rejection Sensitive Dysphoria
Many people and children with ADHD have a heightened sensitivity to perceived rejection. Going back to Freud (Anna Freud), we know one of the most primal defensive reactions is something called projection (you make the other person feel what you don’t’ want to feel). With this in mind, having big (vindictive, angry, irritable) reactions to perceived rejection makes a lot of sense.
Difficulty with Directions
Due to inattention, distractibility, and many more reasons. An ADHD child struggles more with directions. Children diagnosed with ADHD and ODD had more auditory processing difficulties and were shown to be under-responsive to sound. A child who is under-responsive to auditory input doesn’t register noise in the environment as easily and thus may not respond to others when they are speaking. It may appear as if the child is ignoring or disobeying when in fact, they simply have not registered the sound (Ghanizadeh, 2009).
Pathological Demand Avoidance (PDA)
This is a profile that can be present among autists or ADHDers, and is characterized by extreme avoidance of everyday demands and expectations. Essentially, PDA occurs when the person responds to demand with a debilitating anxiety response (think fight-flight-freeze), it demobilizes them. They have an adverse reaction to demands. To learn more about PDA, check out the National Autistic Society and PDA Society.
Implications of Misdiagnosis
As demonstrated above, there are many reasons organic to the ADHD brain that a child may struggle with behaviors that are consistent with an ODD diagnosis. Is it ever helpful to diagnose it? Perhaps it opens up access to parenting training and treatments that help a child better understand and manage intense emotions. However, it’s also possible the diagnosis becomes a self-fulfilling prophecy.
Research on the teacher expectancy effect demonstrates how a teacher’s expectancy of a child influences how the child behaves/performs. This can be detrimental in the context of ODD. I fear that an ODD diagnosis cuts off curiosity; instead of focusing on the why the what gets emphasized. Treatment should focus on the context of the behaviors (family, school, social and cultural contexts). It should consider the child’s sensory experience of the world, the presence of co-occurring mood disorders, and how the child experiences demand, and task-switching.
It is particularly problematic when a child is diagnosed with ODD, and their ADHD is missed, as this leaves them particularly vulnerable. It means they don’t have access to medications, accommodations, certain therapies, and other services to support them better.
A diagnosis of ODD or CD without ADHD occurs more often in BIPOC children and youth. The implications of a misdiagnosis (missing ADHD) place ethnic and racial minority children at additional risk while also perpetuating the disparities that exist “in the medical, educational, and juvenile justice systems” (Fadus et al., 2020). There is a growing body of evidence that unconscious racial bias contributes to this discrepancy in diagnosis. As Fadus et al., 2020 observe:
Some ethnic and racial minority youth are more likely to receive a diagnosis of a disruptive behavior disorder and are less likely to receive a diagnosis of ADHD. When controlling for confounding variables such as adverse childhood experiences, prior juvenile offenses, genetics, and sociodemographics, these diagnostic and treatment disparities remain. Although the cause of these diagnostic disparities is multifactorial, there is concern that unconscious biases may play a role in diagnostic decision-making. As a result of these biases, psychiatrists and trainees may judge and interpret behaviors seen in ODD, CD, and ADHD differently based on race or ethnicity, putting vulnerable populations at risk”.
Clinicians should be aware of the potential for unconscious bias to influence their diagnosis processes and should be diligent about ruling out neurodivergence before diagnosing ODD and other disruptive behavioral disorders. When both co-occur, it is important that parents be supported and that children have access to supports that will help them more easily be able to regulate their emotions and thus their behaviors.
Citations
Ballentine KL. Understanding Racial Differences in Diagnosing ODD Versus ADHD Using Critical Race Theory. Families in Society. 2019;100(3):282-292. doi:10.1177/1044389419842765
Bendiksen, B., Svensson, E., Aase, H., Reichborn-Kjennerud, T., Friis, S., Myhre, A. M., & Zeiner, P. (2017). Co-Occurrence of ODD and CD in Preschool Children With Symptoms of ADHD. Journal of Attention Disorders, 21(9), 741–752. https://doi.org/10.1177/1087054714538655
Fadus, M.C., Ginsburg, K.R., Sobowale, K. et al. Unconscious Bias and the Diagnosis of Disruptive Behavior Disorders and ADHD in African American and Hispanic Youth. Acad Psychiatry 44, 95–102 (2020). https://doi.org/10.1007/s40596-019-01127-6
Ghanizadeh A. Screening signs of auditory processing problem: does it distinguish attention deficit hyperactivity disorder subtypes in a clinical sample of children? Int J Pediatr Otorhinolaryngol. 2009;73:81–87. DOI: 10.1016/j.ijporl.2008.09.020
Kadesjo, C., Hagglof, B., Kadesjo, B., Gillberg, C. (2003). Attention-deficit-hyperactivity disorder with and without oppositional defiant disorder in 3- to 7-year-old children. Developmental Medicine and Child Neurology, 45, 693-699.


")
