
Avoidant Personality Disorder and Autism
The amount of overlap between Autism and AvPD is remarkable enough to give me great pause. It causes me to suspect many high-masking Autistic people are misdiagnosed with AvPD. Over the weekend, I listened to a 4-hour deep dive on social avoidant personality (thank you, @Psychology in Seattle podcast). The whole time I listened, I kept thinking: he’s simply describing the socially motivated, autistic profile!
Contents:
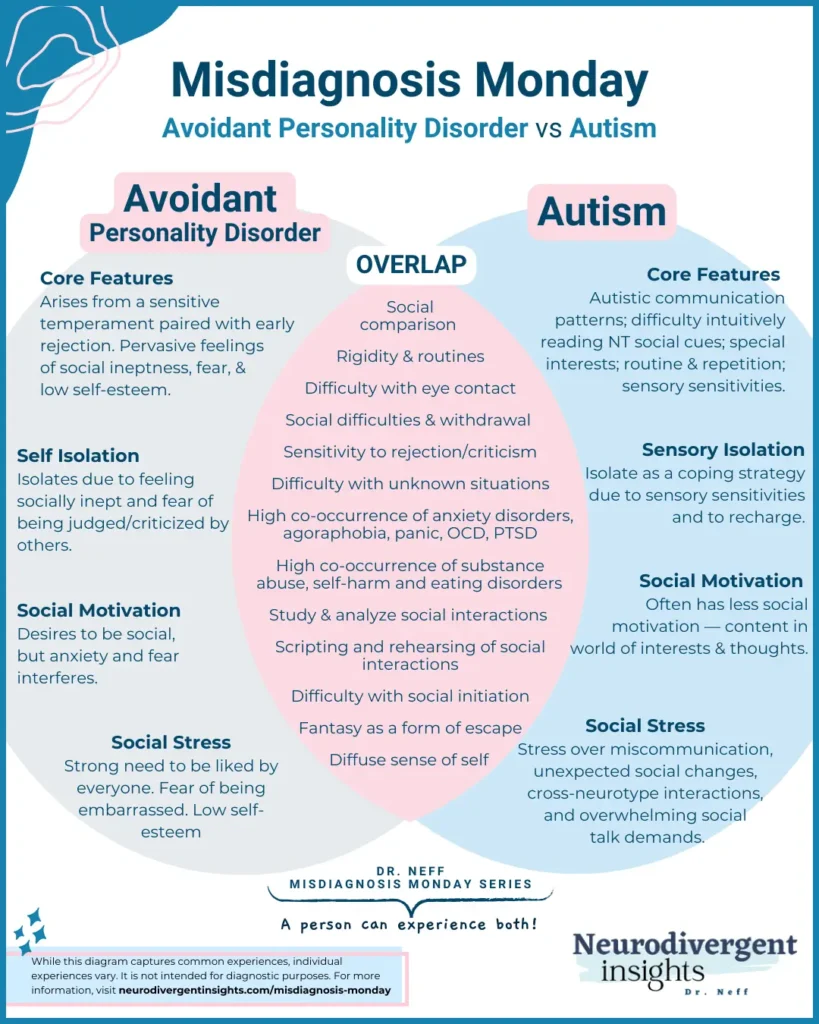
Overlap Between Autism and Avoidant Personality Disorder
There is a lot of overlap between Avoidant Personality Disorder and high-masking autism. We share:
Similar personality traits (low extraversion and high neuroticism)
Similar temperamental traits (difficulty with change and with unexpected changes)
Similar behavioral traits (inhibition and caution)
Overlapping brain circuitry
I suspect avoidant personality becomes one diagnosis commonly used to capture non-stereotypical, undiagnosed Autistic people.
How Outdated Stereotypes Impact Diagnosis
In my research, the information I advise I came across on how to distinguish AvPD from autism relied on outdated stereotypes of autism. For example, Rettew, 2006 suggested:
the socially avoidant person wants social interaction, while the Autistic tends to be happier with independence
the socially avoidant person is hypervigilant to social cues, while the autistic person is under-aware of social cues.
These are based on outdated stereotypes of Autistic people and don’t consider the high-masking, socially motivated autistic profile.
Like many high-masking Autistic people, I am vigilantly aware of people’s body language and facial expressions. I analytically take these in with intensity. And while I am not the most socially motivated autistic (I’m really happy being alone), all of my special interests are relational, and I have deep, existential conversations with people for a living. When the criteria used to distinguish Avoidant Personality from Autism are based on outdated thinking of Autism, I can’t help but wonder how many people diagnosed with Avoidant PD are actually high-masking Autists?
Avoidant Personality Disorder or High-Masking Autism?
Here are a few other things that caught my attention and piqued my curiosity about avoidant personality disorder and its potential relationship to the broader autism phenotype.
It has been noted that symptoms of avoidant personality can be seen as early as age 2. For those who know personality disorder literature, this is wild. Most clinicians won’t diagnose a personality disorder until adulthood. The fact early behavioral and temperamental styles are observed as early as age two reflects the role that temperament and biology play in the development of avoidant personality disorder (McGlashan et al., 2005).
One suspected cause of avoidant personality is “bullying” and rejection from peers. Adults diagnosed with AvPD reported experiencing less popularity, more social isolation, and poorer performance in athletics (Rettew et al., 2003). Autistic children and youth are much more likely to be marginalized and isolated from their peers. They are also more likely to experience dyspraxia which impacts athletic performance. And so, Autism may be one pathway for developing AvPD.
Similar brain circuity has been noted in both conditions. The connection between the amygdala and anterior cingulate gyrus is weaker in both (Velasquez et al., 2017).
A high percentage of eating disorders, rigidity, substance abuse, agoraphobia, OCD, and panic is seen within avoidant personality disorder (Autistics also have similar elevations of these things-see below for statistics).
Overview of Avoidant Personality Disorder
People with Avoidant Personality Disorder (AvPD) experience a pervasive fear of rejection, feelings of inadequacy, and sensitivity to rejection. People with avoidant personality disorder are often plagued with feelings of inadequacy and fear of disapproval. This leads to avoidance of social situations.
Living With Avoidant Personality Disorder
People with Avoidant Personality Disorder tend to have low self-esteem. They live with a chronic sense of inadequacy and fear of criticism. This creates a filter that makes it difficult to perceive things accurately. Because of this overly negative filter they tend to perceive rejection even when it is not there. People with AvPD tend to over-read body language and signals. Neutral signals may be interpreted as signs of being rejected. And minor slights may be experienced in an exaggerated way. This fuels negative self-talk and low-self esteem and perpetuates the avoidance-anxiety spiral.
Complicating matters, the fear of rejection can make talk therapy uncomfortable for people with Avoidant Personality Disorder. When engaged in talk therapy, it may take longer to warm up and feel comfortable with a new therapist. It will be important to establish a strong base of trust and safety with a therapist before engaging in exposure-based work.
Prevalence of Avoidant Personality Disorder
Approximately 1% of the population has socially avoidant personalities. There are unknown causes. However, it is assumed genetics, temperament, environment, and past social experiences are contributing factors (Rettew, 2006).
Time of onset of Avoidant Personality Disorder
Interestingly, while many personality disorders are not diagnosed until adolescence or adulthood, traits and symptoms of avoidance personality disorder can show up much earlier. One study highlighted that symptoms/traits could be seen in children as early as two years old (Rettew et al., 2003).
Social and behavioral inhibition often show up in elementary school. A different study found evidence that high behavioral and harm avoidance levels were connected to a weakened relationship/connectivity between the amygdala and anterior cingulate gyros (which may be related to serotonin transmission) (Velasquez et al., 2017).
Symptoms of Avoidant Personality Disorder
Following is the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria for Avoidant Personality Disorder: A pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, beginning by early adulthood and present in a variety of contexts, as indictated by four (or more) of the following:
1. Avoids occupational activities that involve significant interpersonal contact because of fears of criticism, disapproval, or rejection.
2. Is unwilling to get involved with people unless certain of being liked.
3. Shows restraint within intimate relationships because of the fear of being shamed or ridiculed.
4. Is preoccupied with being criticized or rejected in social situations.
5. Is inhibited in new interpersonal situations because of feelings of inadequacy.
6. Views self as socially inept, personally unappealing, or inferior to others.
7. Is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing.
Other criteria for a diagnosis of avoidant personality disorder is that it must be present since early adulthood and occur in multiple contexts (work, home, social, school, etc.).
Emotional-Social Experience of Avoidant Personality Disorder
The emotional experience of avoidant personality disorder includes excessive self-consciousness and anxiety in everyday social situations, extreme fear of being watched or judged by others, fear that others will notice that you’re nervous or see you embarrassed (blushing), fear of being humiliated, and intense worry and rumination before an upcoming social situation.
While there is no clear data on the co-occurrence of Autism and AvPD, many professionals within the Autism community believe that AvPD occurs more often among autistic adults. Reasons may include (Source):
Experiencing social rejection and bullying as a child
Diffuse employment difficulties
Difficulty cultivating and maintaining friendships
I would add that I suspect AvPD may be high among undiagnosed Autistics for the following reason:
A sense of being “different” but without having a known cause/name for the difference may lead to a sense of being “inept” or “discovered.”
Hypervigilance to other’s reactions as a form of masking
Social isolation and difficulty blending in but with an unknown cause/reason
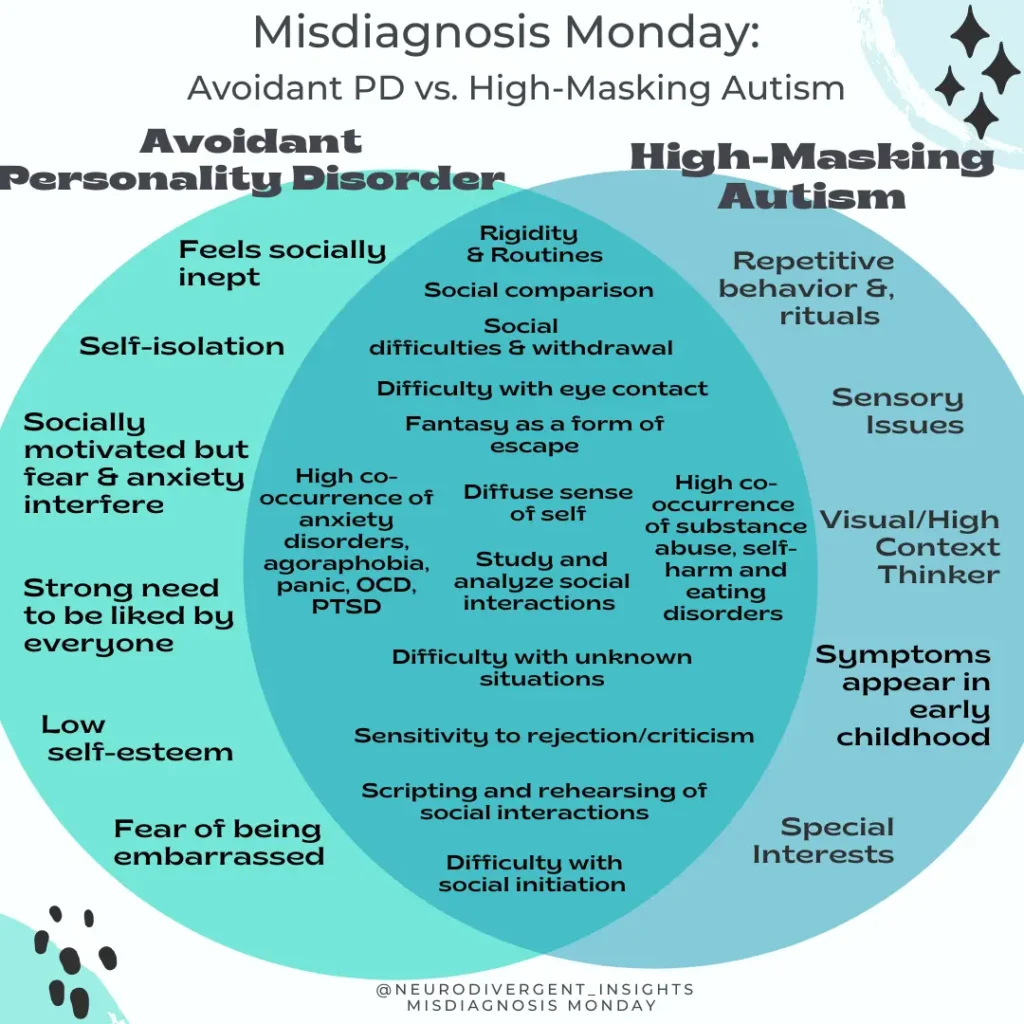
Overlapping Traits between AvPD and Autism
Intensive fear of/sensitivity to criticism and rejection
This is one of the core criteria of AvPD. This can also be common for many high-masking autistics. Rejection Sensitivity Dysphoria is common among both ADHDers and Autistics. RSD is characterized by intense sensitivities to rejection and criticism. Both groups often live with an intense fear of criticism.
Social Withdrawal/Tendency to Stay Home
There is a strong aversion to being in public for the avoidant personality. It is largely related to the fear of being evaluated/judged or doing something embarrassing. For the Autistic, it may be due to the energy cost of being around others/preference for being alone/due to sensory issues.
Hypervigilant Awareness of Social Cues
For the avoidant personality, they will be hypervigilant about body cues of others and often misread these as more negative than they actually are. For the high-masking autistic, because we don’t intuitively pick up on body-based social cues, we often learn to analytically attend to these social cues and often do so with hypervigilance.
A Diffuse Sense of Self
Another core feature of Avoidant PD is a diffuse sense of self/feeling unknown to oneself. Masking comes at the cost of a lack of social identity. With masking, a person is often contorting and shapeshifting to the needs of others. This comes at the cost of having a diffuse connection to oneself.
Difficulty with New Situations/Preference for Routine
Both groups experience stress and difficulty navigating new social situations, and both prefer sticking with the known, familiar, and routine.
Shared Risks/Co-Occurrence
We share many similar risks of co-occurring conditions, from PTSD to OCD to substance abuse.
OCD
Both AvPD and Autism have higher prevalence rates of OCD.
The co-occurrence prevalence of OCD and AvPD ranges from 5-15% (Thamby & Khanna, 2019).
Van Steensel et al. (2011) meta-analysis found that 17% of Autistic young people also had OCD.
47% of people with OCD had clinically significant Autistic traits, and 27.8% met full diagnostic criteria for Autism. It is speculated that a larger proportion of people with OCD may also have Autism (Wikramanayake et al., 2018).
A population-based study done in Denmark (Meier et al., 2015) found
Autistics were 2x more likely to be diagnosed with OCD later in life.
People diagnosed with OCD were 4x more likely to be diagnosed with Autism later in life.
Substance Abuse
In Langås et al. 2012 study, 46 percent of patients with a substance abuse disorder had a co-occurring personality disorder. Of the 46 percent, 8 percent had AvPD.
Substance abuse is also common among autistics with average to high IQ. A recent study in Sweden found that folks with Autism with average to high IQs were twice as likely to struggle with addiction to alcohol or other drugs.
Self-Harm
Gratz and Tull, 2012 found elevated self-harm among people who had AvPD + PTSD (even more so than those with BPD + PTSD). Similarly, self-harm is high among autistics with average to high IQs.
One study found that parents reported self-harm behavior among autistic youth in 15% of cases (Huang).
Eating Disorders
Diaz-Marsa and Saiz, 2000 found high provenance rates of people with Avoidant Personality disorder among patients with anorexia nervosa.
Anorexia nervosa is also common among autistic AFAB/women. While the rates vary, most researchers agree that about 23% of people diagnosed with anorexia nervosa are Autistic. However, many agree, that this is likely an underrepresentation due to the fact ASD often goes undiagnosed within this population (Westwood and Tchanturia)
Generalized Anxiety
High rates of generalized anxiety and other anxiety disorders have been noted within AvPD (findings range from 35%-100%, Marques et al., 2012).
Approximately 40% of Autistics also meet the criteria for an anxiety disorder (Zaboski and Storch, 2018).
Depression
One study found that among 243 patients with depression, 28.4% met the criteria for AvPD (compared to 1% of the general population). (Alpert et al., 1997).
Depression also commonly co-occurs among Autistic individuals. Lainhart and Folstein, 1994 found that approximately 1/3 of autistic teens and adults had at least one episode of major depression within their lifetime.
How to Spot the Difference between Avoidant Personality Disorder and Autism?
Given the high degree of overlap, spotting the difference can be quite difficult. Here are a few of my guidelines for clinicians providing services and assessments:
When assessing for AvPD (or any personality disorder!) Autism should be on the rule-out list.
Consider using routine screeners for Autism (such as the AQ, CAT-Q, and RAADS)
Focus on criteria B for Autism (there will be a lot of overlap between criteria A for Autism and AvPD).
Gather a thorough developmental history and listen for subtle signs of Autism
Understand their sensory experience of their world (ask direct questions to help those who internalize).
Ask about their areas of special interest. For an Autistic person, you will feel as if you are contacting them and will likely notice a change in effect, openness, verbal fluency, and more.
For more in-depth guidance on how to spot the difference, see my Autism vs. Avoidant Personality Disorder e-book.
Citations:
ALPERT, J., UEBELACKER, L., McLEAN, N., NIERENBERG, A., PAVA, J., WORTHINGTON III, J., . . . FAVA, M. (1997). Social phobia, avoidant personality disorder and atypical depression: Co-occurrence and clinical implications. Psychological Medicine, 27(3), 627-633. doi:10.1017/S0033291797004765
Butwicka, A., Långström, N., Larsson, H. et al. Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study. J Autism Dev Disord 47, 80–89 (2017). https://doi.org/10.1007/s10803-016-2914-2
Díaz-Marsá, M., Carrasco, J. L., & Sáiz, J. (2000). A study of temperament and personality in anorexia and bulimia nervosa. Journal of personality disorders, 14(4), 352–359. https://doi.org/10.1521/pedi.2000.14.4.352
Gratz, K. L., & Tull, M. T. (2012). Exploring the relationship between posttraumatic stress disorder and deliberate self-harm: The moderating roles of borderline and avoidant personality disorders. Psychiatry research, 199(1), 19-23.
Hurley RS, Losh M, Parlier M, Reznick JS, Piven J. The broad autism phenotype questionnaire. J Autism Dev Disord. 2007 Oct;37(9):1679-90. doi: 10.1007/s10803-006-0299-3. Epub 2006 Dec 5. PMID: 17146701.
Lainhart JE, Folstein SE. Affective disorders in people with autism: a review of published cases. J Autism Dev Disord 24:587-601, 1994
Langås, A. M., Malt, U. F., & Opjordsmoen, S. (2012). In-depth study of personality disorders in first-admission patients with substance use disorders. BMC psychiatry, 12, 180. https://doi.org/10.1186/1471-244X-12-180
Marques, L., Porter, E., Keshaviah, A., Pollack, M. H., Van Ameringen, M., Stein, M. B., & Simon, N. M. (2012). Avoidant personality disorder in individuals with generalized social anxiety disorder: what does it add?. Journal of anxiety disorders, 26(6), 665–672. https://doi.org/10.1016/j.janxdis.2012.05.004
McGlashan, T. H., Grilo, C. M., Sanislow, C. A., Ralevski, E., Morey, L. C., Gunderson, J. G., Skodol, A. E., Shea, M. T., Zanarini, M. C., Bender, D., Stout, R. L., Yen, S., & Pagano, M. (2005). Two-year prevalence and stability of individual DSM-IV criteria for schizotypal, borderline, avoidant, and obsessive-compulsive personality disorders: toward a hybrid model of axis II disorders. The American journal of psychiatry, 162(5), 883–889. https://doi.org/10.1176/appi.ajp.162.5.883
Rettew, D. C., Zanarini, M. C., Yen, S., Grilo, C. M., Skodol, A. E., Shea, M. T., McGlashan, T. H., Morey, L. C., Culhane, M. A., & Gunderson, J. G. (2003). Childhood antecedents of avoidant personality disorder: a retrospective study. Journal of the American Academy of Child and Adolescent Psychiatry, 42(9), 1122–1130. https://doi.org/10.1097/01.CHI.0000070250.24125.5F
Rettew, D. C. (2006). Avoidant Personality Disorder: Boundaries of a Diagnosis. Psychiatric Times, 23(8), 38-38. Retrieved at: https://www.psychiatrictimes.com/view/avoidant-personality-disorder-boundaries-diagnosis
Thamby, A., & Khanna, S. (2019). The role of personality disorders in obsessive-compulsive disorder. Indian journal of psychiatry, 61(Suppl 1), S114–S118. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_526_18
Velasquez, F., Wiggins, J. L., Mattson, W. I., Martin, D. M., Lord, C., & Monk, C. S. (2017). The influence of 5-HTTLPR transporter genotype on amygdala-subgenual anterior cingulate cortex connectivity in autism spectrum disorder. Developmental cognitive neuroscience, 24, 12–20. https://doi.org/10.1016/j.dcn.2016.12.002
Westwood, H., Tchanturia, K. Autism Spectrum Disorder in Anorexia Nervosa: An Updated Literature Review. Curr Psychiatry Rep 19, 41 (2017). https://doi.org/10.1007/s11920-017-0791-9
Zaboski, B. A., & Storch, E. A. (2018). Comorbid autism spectrum disorder and anxiety disorders: a brief review. Future neurology, 13(1), 31–37. https://doi.org/10.2217/fnl-2017-0030


")
