Updated March 17, 2026
When a Black or Brown child sits down in front of a clinician, what, exactly, is that clinician seeing? When that same child can’t stay in their seat or avoids homework, what does the teacher see?
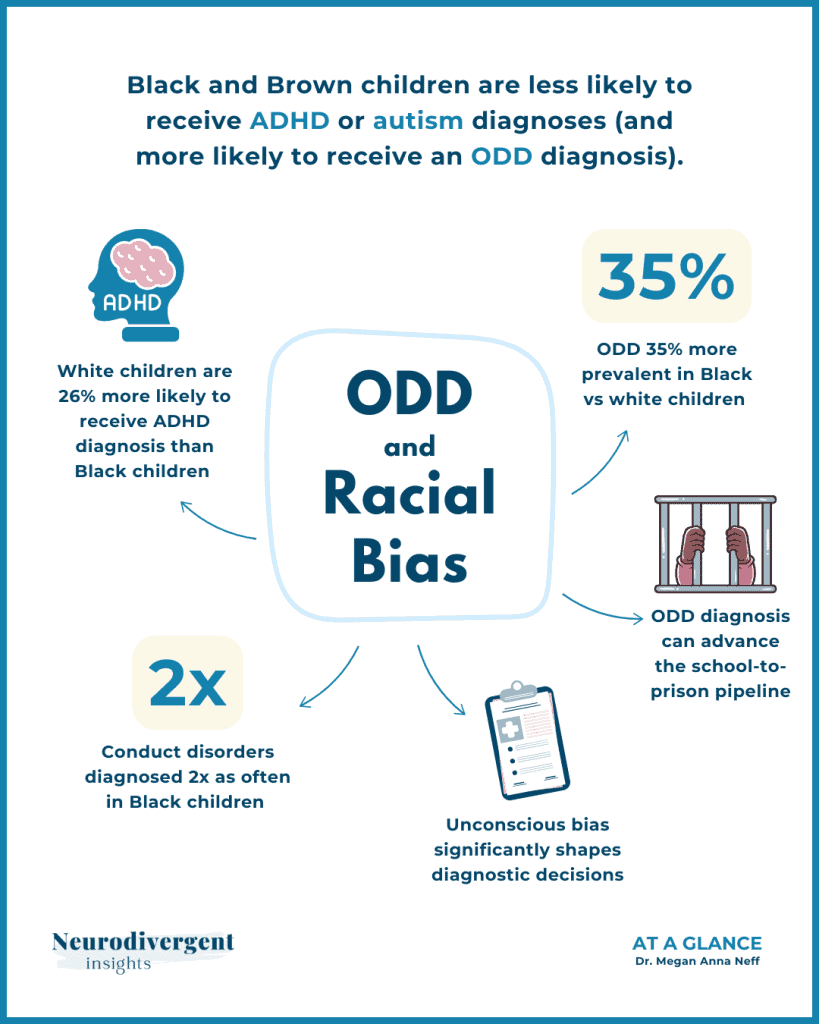
The questions are not hypothetical; the research gives us an uncomfortable answer. The same behaviors that earn a white child an ADHD or an autism diagnosis and a referral for support often earn a Black or Brown child an ODD label and a path toward punishment. This is not a fringe concern; it is one of the most well‑documented disparities in child mental health.
And as a neurodivergent clinician, it sits heavy with me. Because I know how much a diagnosis shapes a life. A single word on a chart can can open doors to understanding, accommodation, and self-compassion. The wrong one can open doors to harmful treatments, shame and character-based labels.
Table of Contents
What the Data Shows: ODD Overdiagnosis and ADHD Underdiagnosis in BIPOC Children
The pattern is consistent across studies, and it has only grown clearer in the last few years with larger datasets.
A 2024 analysis of more than 849,000 ADHD patients and 157,000 conduct disorder patients across 50 U.S. health care organizations found that white children were about 26% more likely to receive an ADHD diagnosis than Black children, while Black individuals were 61% more likely to be diagnosed with conduct disorder; ODD was also 35% more prevalent in Black patients than white patients. In the same dataset, conduct disorders were diagnosed more than twice as often in Black children as in white children (Williams et al., 2024).
A separate national analysis of more than 700,000 pediatric hospitalizations found that racially minoritized children were consistently more likely than white children to receive a disruptive behavior disorder diagnosis (Lugo-Candelas et al., 2024):
- American Indian/Alaska Native children had 2.18 times the odds,
- Asian children 1.88 times the odds
- Black children 1.40 times the odds
- Hispanic children 1.20 times the odds
These studies are not perfect, and they cannot tell us everything about individual children, but together they paint a disturbingly consistent picture of who gets seen as “ADHD” and who gets labeled “disruptive.
What the newest numbers show
Recent national data from the CDC show that ADHD diagnoses have climbed overall: about 13% of white children, 11% of Black children, and 9% of Hispanic children ages 5 to 17 now have an ADHD diagnosis on record.
And while the racial gap has narrowed compared to earlier estimates, it has not disappeared—and the direction of the gap still matters. White children remain more likely to be recognized as having ADHD, while Black and Brown children are still more likely to have similar behaviors interpreted as “behavior problems” and coded as disruptive behavior disorders instead.
Even when researchers account for things like exposure to adversity, prior juvenile justice involvement, and socioeconomic differences, race still predicts who gets which label. That data provides us with a window into how behavior is seen through a racialized lens.
What Drives These Disparities: Bias, Perception, and History
Clinicians do not diagnose in a vacuum. They carry implicit biases shaped by the same culture that produces racial inequity everywhere else. Research has consistently shown that clinicians tend to over-pathologize the behaviors of Black and Brown children, reading defiance and danger where they might read dysregulation or distress in a white child (Fadus et al., 2020).
A striking 2025 paper in Pediatrics by Legha draws a historical through-line that I think every clinician should be aware of. From drapetomania in 1851, a diagnosis invented to pathologize enslaved people who sought freedom, to “protest psychosis” during the Civil Rights era, to the modern overdiagnosis of ODD in Black children, there is a pattern of psychiatry framing resistance to unjust conditions as pathology (Legha, 2025).
That is a difficult lineage to hold. But I think we need to hold it.
Legha also names adultification bias: the documented tendency of adults to perceive Black children as stronger, more adult-like, and less innocent than their white peers. When a seven-year-old Black girl pushes back on a classroom instruction, adultification bias can transform that moment from a child having a hard time into a child being defiant. Black girls are suspended at five times the rate of white girls (Legha, 2025).
And here is what troubles me most as a neurodivergent clinician: ODD, by design, pathologizes behaviors as features of the child rather than manifestations of neurodevelopmental difference, trauma, or environmental mismatch. It locates the problem in the child. When applied disproportionately to BIPOC children, it becomes, as Legha argues, a functionally racist diagnostic practice.
The Neurodevelopmental Overlap Clinicians Are Missing
There’s another layer to this conversation about ODD and racial bias that often gets missed, and it matters.
ADHD and ODD co-occur at very high rates. Among children with ADHD-Combined presentation, approximately 53% also meet criteria for ODD. When autism co-occurs with ADHD-Combined (what many of us call AuDHD), that number rises to 62% (Mayes, 2025). In other words, the behaviors that get labeled as “oppositional” are often expressions of neurodevelopmental differences: sensory overwhelm, demand avoidance, executive function challenges, or the kind of rigid-flexible mismatch that comes with being Autistic in environments designed for neuronormative compliance.
This matters for the racial bias conversation because of a framing disparity playing out in clinical settings. When a white child shows persistent demand avoidance, there is a growing tendency to consider a PDA (Pathological Demand Avoidance) profile, an empathetic, neurodevelopmental framing. When a Black or Brown child shows similar behaviors, the path too often leads to ODD, a punitive, behavioral framing.
Same behaviors, radically different stories. Instead of asking what needs are going unmet, the child is steered into behavior plans and consequences. Those stories don’t just describe a child; they often shape a trajectory.
And the research itself reflects these blind spots. A 2024 review of conduct disorder literature screened 2,791 manuscripts published between 2013 and 2023. Only 136 were original research with diagnostic data, and of those, only 13 contained any racial or ethnic data at all. Racism was rarely mentioned as a potential explanation for disparities (Brown et al., 2024). We are not just failing to address this clinically, we are also failing to even study it adequately.
The Downstream Harm: Treatment Access and the School-to-Prison Pipeline
A misdiagnosis does not just sit on paper. It shapes what happens next.
When a child’s ADHD is missed and they receive an ODD diagnosis instead, they lose access to the medications, therapies, and educational accommodations that could support their actual neurodevelopmental needs. In schools, they are more likely to be written up than supported, disciplined rather than accommodated, suspended rather than scaffolded.
The treatment access numbers are sobering; white children with ADHD have about a 1 in 2 chance of getting treatment in a given year; for Black children, that probability drops by 15%, for Hispanic children by 12%, and for Asian children by 21% (Yang, 2024). What stands out is that these gaps are driven mostly by barriers to getting in the door in the first place, not by a lack of interest in treatment once it is available.
Child psychiatrist Rupi Legha connects this directly to the school‑to‑prison pipeline. An ODD diagnosis does not stay in the clinic; it follows a child through their school record, shaping how teachers and administrators see them, interact with them and how quickly discipline escalates. For Black children, being filtered through a behavioral lens means more suspensions, more expulsions, and more contact with the juvenile justice system, with the diagnosis functioning like another cog in the machinery.
I want to be careful here, because I don’t believe most clinicians intend harm. But intent does not undo impact. When we diagnose without looking squarely at our own biases — the ones we’ve been inhaling just by living in these systems — we become part of a machine that compounds harm for the children who are already most vulnerable.
Confronting Racial Bias in Mental Health: What Needs to Change
Legha (2025) proposes a three-step antiracist framework that I find both practical and honest:
- First, connect to racism’s legacy. Clinicians need to understand the historical through-line of psychiatric diagnoses used to pathologize Black resistance. Not as an abstract history lesson, but as context that actively shapes the diagnostic encounter happening right now.
- Second, diagnose the racism. Before diagnosing ODD, clinicians should rigorously consider ADHD, autism, mood and anxiety disorders, PTSD, and adjustment disorders. They should ask whether the child’s environment, not the child’s character, might explain the behavior.
- Third, antiracist psychoeducation, documentation, and activism. This means educating families about their rights, documenting disparities when observed, and advocating for systemic change within the institutions we work in.
I would add something from my own perspective as a neurodivergent clinician: we need to widen the frame of what we consider when a child is struggling. Neurodevelopmental differences, sensory needs, demand avoidance, PDA, executive function challenges. These are not defiance. And when we collapse them into a behavioral diagnosis, we lose the child.
I do not have a clean ending for this, because there is no clean ending. The disparities are structural, and they are ongoing. Children are being harmed by them right now.
But I believe that naming what is happening is the first step. And I believe that clinicians who care enough to read something like this are also clinicians who can do something different in the room, the next time a Black or Brown child sits in front of them and is struggling.
Follow-Up Resources
Recommended Reading and Trainings
It’s Never Just ADHD: Finding the Child Behind the Label by Sandra Coral is a great read for educators (or child clinicians) seeking to more deeply understand ADHD through an intersectional lens.
For culturally responsive trainings on the intsersection of neurodevelopmental conditions and BIPOC realities check out the work of Living Autism Outloud.
Stay in the Neurodivergent Loop
For ongoing insights and updates, subscribe to the Neurodivergent Insights Newsletter. Each Sunday, I send out fresh thoughts and a roundup of the newest resources on topics related to neurodivergence, mental health, and wellness. My most personal writing is reserved for my newsletter, and subscribers also get access to the newsletter vault (12+ PDFs) when they join.
References
Ballentine KL. Understanding Racial Differences in Diagnosing ODD Versus ADHD Using Critical Race Theory. Families in Society. 2019;100(3):282-292. doi:10.1177/1044389419842765
Brown, N. M., et al. (2024). Reporting of race and ethnicity in conduct disorder literature. Psychiatric Research and Clinical Practice, 6(3). https://doi.org/10.1176/appi.prcp.20240009
CDC National Center for Health Statistics. (2024). Data Brief No. 499: Attention-deficit/hyperactivity disorder in children ages 5-17 years, 2020-2022. https://www.cdc.gov/nchs/products/databriefs/db499.htm
Cameron M, Guterman N. Diagnosing conduct problems of children and adolescents in residential treatment. Child Youth Care Forum. 2007;36(1):1–10.
Coker, T. R., Elliott, M. N., Toomey, S. L., Schwebel, D. C., Cuccaro, P., Tortolero Emery, S., Davies, S. L., Visser, S. N., & Schuster, M. A. (2016). Racial and Ethnic Disparities in ADHD Diagnosis and Treatment. Pediatrics, 138(3), e20160407. https://doi.org/10.1542/peds.2016-0407
Fadus, M.C., Ginsburg, K.R., Sobowale, K. et al. Unconscious Bias and the Diagnosis of Disruptive Behavior Disorders and ADHD in African American and Hispanic Youth. Acad Psychiatry 44, 95–102 (2020). https://doi.org/10.1007/s40596-019-01127-6
Hu, X., & Morgan, P. L. (2023). Sociodemographic disparities in ADHD among elementary schoolchildren. Psychiatry Research, 327, 115393. https://doi.org/10.1016/j.psychres.2023.115393
Legha, R. (2025). There are no bad kids: An antiracist approach to oppositional defiant disorder. Pediatrics, 155(2), e2024068415. https://doi.org/10.1542/peds.2024-068415
Lugo-Candelas, C., Shah, R., Saint-Hilaire, S., & Savage, J. (2024). Racial disparities in disruptive behavior disorder diagnosis among pediatric inpatients. Frontiers in Psychiatry, 15. https://doi.org/10.3389/fpsyt.2024.1425559
Mayes, S. D., Pardej, S. K., & Waschbusch, D. A. (2025). Oppositional defiant disorder in autism and ADHD. Journal of Autism and Developmental Disorders, 55, 4092–4105. https://doi.org/10.1007/s10803-024-06437-9
Morgan PL, Staff J, Hillemeier MM, et al. Racial and ethnic disparities in ADHD diagnosis from kindergarten to eighth grade. Pediatrics. 2013;132(1):85–93.
Shi Y, Hunter Guevara LR, Dykhoff HJ, et al. Racial Disparities in Diagnosis of Attention-Deficit/Hyperactivity Disorder in a US National Birth Cohort. JAMA Netw Open. 2021;4(3):e210321. doi:10.1001/jamanetworkopen.2021.0321
Sloat, E. R., Torres-Pagán, L., & Gornik, A. (2023). Race and mental representation of ODD. Journal of Social and Clinical Psychology, 42(4), 365-385. https://doi.org/10.1521/jscp.2023.42.4.365
Williams, A., Shalaby, R., & Sengupta, A. (2024). Large-scale analysis of racial disparities in ADHD and conduct disorder. Scientific Reports, 14. https://doi.org/10.1038/s41598-024-75954-5
Yang, K. G., Flores, M. W., et al. (2022). Racial and Ethnic Disparities in Childhood ADHD Treatment Access and Utilization: Results From a National Study. Psychiatric Services, 73(12), 1338-1345.
More Like This...


Previous Graphics