Let's Start With a Conversation
If you’ve found yourself wondering what’s going on with the rising numbers of autism diagnoses — especially after hearing headlines about an “autism epidemic” — you’re not alone.
This is one of those topics that stirs up a lot for many in our community: confusion, fear, curiosity, even anger. And understandably so. For decades, autism was portrayed as something rare and tragic — something that stole children away from their families.
Now, many of us are discovering we’ve been Autistic all along — raising Autistic kids, working alongside Autistic colleagues, or slowly peeling back the layers of our own identities and realizing: Oh … this is me.
Many of us (though not all) embrace this as a valid identity — one we don’t feel needs to be cured. Which is why these narratives can understandably activate our threat response, crowd in on our sense of safety, and spark our activism energy.
I’m a big context person. I find it grounding to step back — to understand the historical moment, the social conditions, and the layered textures we’re all moving within. So that’s what I’ll offer here: some context. And maybe, through that, a bit of clarity around these questions that keep coming up.
Table of Contents
Why Are Autism Diagnoses on the Rise?
So, what changed?
Did something in the environment shift? Is autism becoming more common? Or are we simply getting better at recognizing something that’s always been here?
Before we dive into the data, I want to pause on something that often gets lost in these conversations:
Autism is not new. Recognition is.
And the way we talk about this matters — especially when public figures use phrases like “autism epidemic,” framing our existence as a crisis to be solved.
What if we told a different story?
Not one rooted in fear or urgency, but one grounded in context — in history, science, systems, and lived experience. That’s what I hope to offer here. A chance to zoom out, to slow the spiral of misinformation, and to look with clarity and care at what’s actually driving these numbers.
Because this isn’t just about data. It’s about people. And for many of us — including myself — it’s a story we’ve lived in our bodies long before it showed up on a chart.
So let’s begin.
Is There Really an Autism Epidemic?
Let’s address the elephant in the headline: RFK Jr. recently called autism a “catastrophic epidemic” and pledged to find its cause by September. This kind of language may grab attention, but it distorts reality — and often causes real harm along the way.
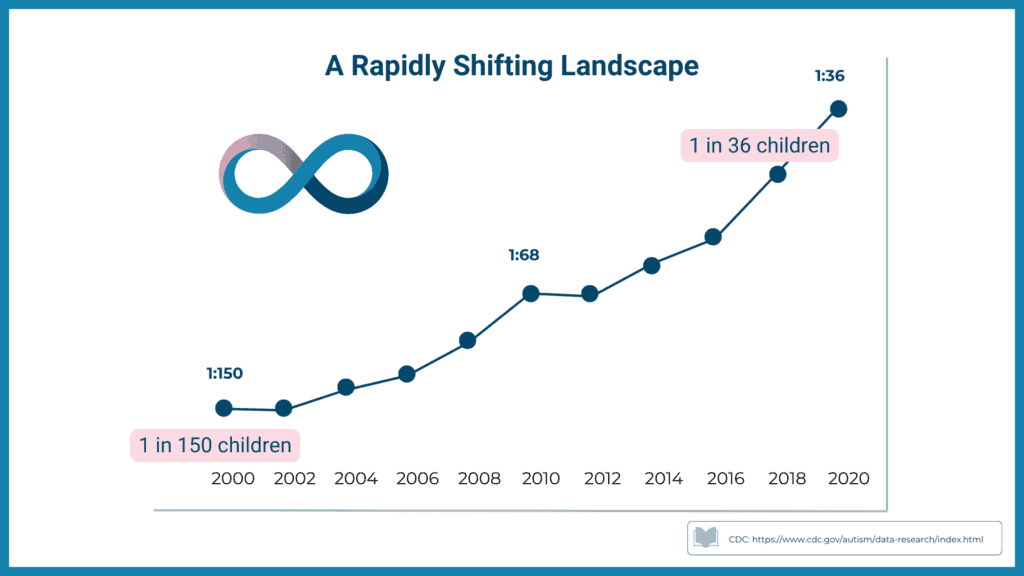
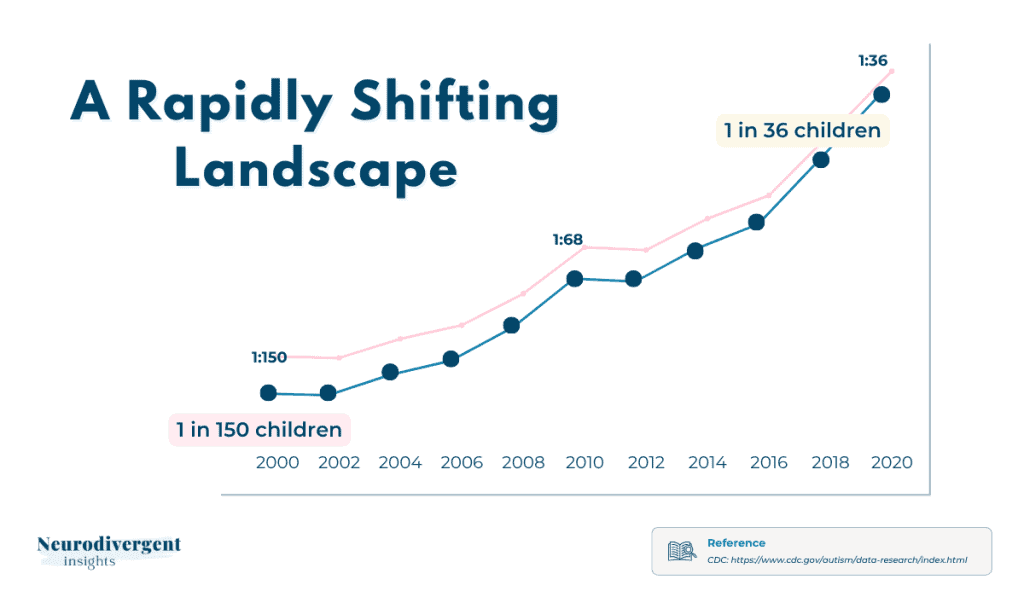
First, let’s be clear about the data. Yes, autism diagnoses have increased over the past few decades. Dramatically so. The CDC now estimates that 1 in 36 children in the U.S. are identified as Autistic. That’s a steep climb from the 1 in 2,500 estimate just a few generations ago (CDC, 2024).
But numbers don’t tell the whole story.
This isn’t a case of autism suddenly spreading like a virus. (We’re not in the middle of some special interest–ravaged pandemic.) It’s a case of finally putting the right name to an experience that’s always been here — but was previously misdiagnosed, misunderstood, or missed altogether.
Calling it an epidemic suggests contagion, pathology, a crisis to be solved. But what if what we’re actually seeing is a long-overdue correction? What if this “epidemic” is really a reckoning with how narrowly we’ve defined autism in the past?
The truth is, we’ve radically shifted the way we define, diagnose, and even think about autism — especially in the last 30 years. We’ve moved away from a rigid, deficit-based view and toward a broader, spectrum-based understanding that includes a wide range of experiences and support needs.
That shift matters. It means more people are getting identified — not because autism is suddenly appearing out of nowhere, but because our frameworks have changed. Our context has changed, and that’s reflected in the numbers we see.
So when RFK Jr. frames this as a mystery to solve or a crisis to stop, it misses the point. Autism isn’t something we’re catching. It’s something we’re recognizing — often for the first time, in ourselves or in the people we love.
And that recognition?
For many of us, it isn’t catastrophic. It’s clarifying. It’s naming something that’s been there all along. It’s relief. It’s resonance. It’s the beginning of understanding.
And for some … it’s more complicated than that.
For some, discovering they — or their child — is Autistic brings grief, fear, or uncertainty alongside the insight. It can stir up questions about support, about belonging, about how life might need to change. The meaning of diagnosis often unfolds slowly, shaped by each person’s context, needs, and access to care.
So while many of us experience this recognition as a kind of homecoming, others may feel like they’ve just stepped into unfamiliar terrain. Both experiences are valid. And both deserve space in this conversation.
But back to history — and back to the story of autism.
Because to understand where we are now, we need to understand where we’ve been.
A Brief History of Autism
Before autism had a name, it had always been here.
Because autism didn’t start with the DSM.
The traits we now recognize as Autistic — deep focus, sensory intensity, pattern recognition, social divergence — have been part of the human story for millennia. Long before diagnostic manuals. Long before “awareness months.”
Some researchers even trace these traits back to the Ice Age.
Cave art found across Europe — especially in the Chauvet and Lascaux caves in France, and Altamira in Spain — have led to speculation that these layered, detailed animal depictions may have been created by Autistic minds (Humphrey, 1998; Spikins, 2018). The kind of attention to detail, pattern, and movement we now associate with autism could have been a gift to early human communities: helping track animals, understand rhythms of nature, or express meaning beyond language.
Fast forward a few thousand years, and we begin to see these traits show up in written form. In ancient Mesopotamia, clay tablets described people with a distinct communication styles, intense interests, and different social rhythms. Some were seen as wise or spiritually gifted. Others were cast out.
Which reminds us: neurodivergence has never been just about biology. It’s also about how culture makes meaning of difference.
From Autism in the 20th Century
It wasn’t until the early 20th century that autism began to emerge as a medical category. The term itself was first coined by Swiss psychiatrist Eugen Bleuler in the early 1900s to describe a withdrawal into one’s inner world — what he observed in patients with schizophrenia. For decades, autism would remain entangled with schizophrenia.
It wasn’t until the 1940s that clinicians like Leo Kanner and Hans Asperger began describing autism as a distinct condition. Kanner called it “early infantile autism,” framing it as an inborn difference in emotional connection and communication. Asperger described “autistic psychopathy,” observing children with more fluent language but notable challenges in social reciprocity and focused interests.
Still, both of their early definitions were narrow — centered on white boys with visible, externalized traits and limited variation in communication or support needs. And because of that, many of us were never even considered.
And they weren’t the first.
Russian psychiatrist Grunya Sukhareva had published detailed case studies of autistic children nearly two decades earlier — describing sensory sensitivities, focused interests, and even gender differences in how autism presents. But her work was overlooked in Western research for most of the 20th century.
It feels fitting, in a bittersweet way, that one of the first to document autism was a woman — whose work, like so many Autistic, remained hidden in plain sight.
That early framing — who got seen, who didn’t, and who got written out — shaped public perception for decades.
That’s how the stereotype took root.
But then it got more complicated.
Shortly after Kanner’s research took off, so did psychodynamic and family systems theory — schools of thought that viewed psychological difference through the lens of relational or emotional wounding. In that context, autism began to be seen not as a natural neurodevelopmental difference, but as a response to parental failure.
Kanner himself observed that many parents of Autistic children appeared emotionally distant, and in a 1949 paper, he speculated whether this detachment might be contributing to the child’s behaviors (Kanner, 1949). His observations weren’t meant as blame — but they laid the groundwork for what came next.
In the 1950s, psychoanalyst Bruno Bettelheim expanded on these ideas and popularized what became known as the “refrigerator mother” theory: the belief that autism was caused by cold, unloving mothers who failed to properly bond with their children (Waltz & Shattock, 2004).
And with that, the stigma deepened. It became shameful to have an Autistic child — because it pointed to the fact you were cold, withholding, or even to blame.
And I can’t help but wonder — how many of those mothers were undiagnosed autistic themselves?
Not cold. Just different.
Offering love and connection in quieter, more private ways that didn’t match neurotypical expectations.
But in a world that couldn’t see those gestures for what they were, misunderstanding turned into myth.
That’s how the stereotype took root. And then how the stigma grew.
From Misunderstood to Miscounted
How stigma, stereotypes, and a narrow lens shaped who got seen — and who didn’t.
That early misunderstanding didn’t just stick. It snowballed — shaping decades of diagnostic practices and public perception.
Autism became defined in narrow terms that excluded most of us. Girls, genderqueer people, people of color, adults, and anyone whose traits weren’t overt or disruptive enough — we were overlooked. Misdiagnosed. Or left wondering why life always felt just a bit off-script.
It wasn’t until the 1990s that the idea of autism as a spectrum entered the clinical conversation. And only in the past two decades have we begun to see more expansive definitions — ones that include those of us on the “invisible” end of the spectrum: those who masked, coped, compensated, or collapsed in silence.
This matters, because when people ask, “Why are autism rates going up?” — part of the answer is this:
We’ve widened the lens. We’ve expanded the definition. And we’ve begun to recognize what was already there.
So, no — autism isn’t a modern epidemic.
It’s a long-running story that’s just now getting a fuller telling.
What is Causing High Rates of Autism?
(Spoiler: It’s not an epidemic. It’s recognition catching up to reality.)
Let’s take a closer look at a question that comes up again and again — “What is causing the rise in autism?”
Depending on who you ask, you might hear anything from environmental toxins to screen time to conspiracy theories about vaccines. But the real answer is simpler — and more hopeful. What we’re seeing isn’t a surge in autism itself. It’s a shift in how we define it, recognize it, and respond to it.
In other words, diagnoses are going up because recognition is finally catching up to reality.
Here are five key reasons why:
#1: Broadening Diagnostic Criteria
The Diagnostic Criteria Changed — A Lot
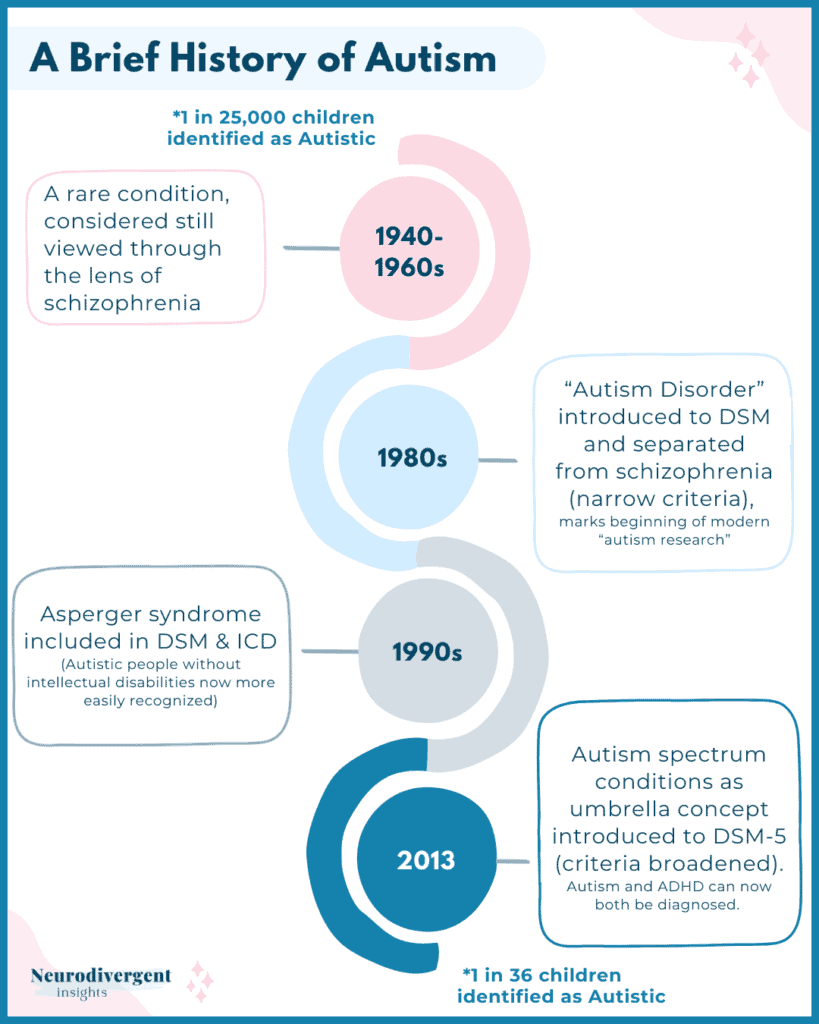
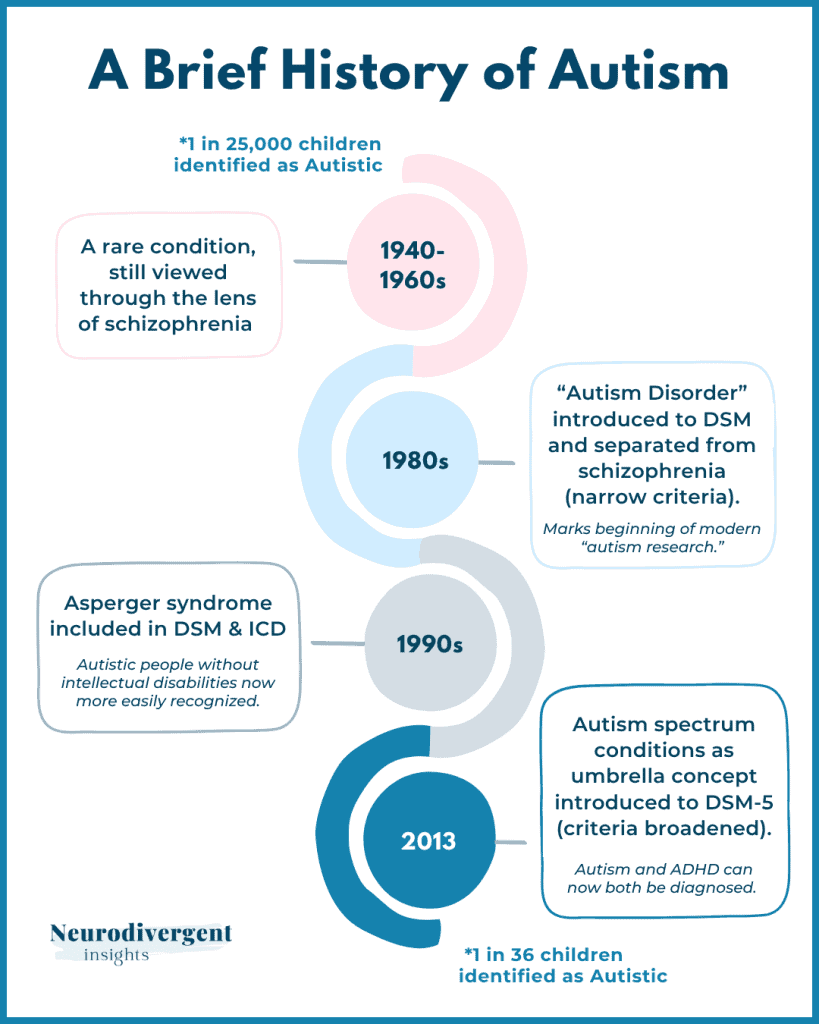
Autism wasn’t recognized as its own diagnostic category until the 1980s. Before then, Autistic people were often misdiagnosed with childhood schizophrenia — or simply overlooked altogether.
The shift began with the DSM-III in 1980, which was the first to list autism as a distinct neurodevelopmental disorder. For the first time, autism was recognized as its own diagnostic category — separate from childhood schizophrenia and no longer buried under vague behavioral labels.
This shift was huge. It meant that Autistic individuals could begin to be understood on their own terms, rather than being miscast in diagnostic categories that didn’t quite fit. It also marked the beginning of modern autism research and clinical recognition — though the criteria remained narrow, based largely on observable traits in young children, especially white, cisgender boys, whose presentation shaped early diagnostic norms.
From there, the definitions continued to evolve:
- 1994: The DSM-IV expanded the criteria to include Asperger’s Syndrome and PDD-NOS, allowing more individuals — especially those without intellectual disabilities — to be recognized.
- 2013: The DSM-5 unified these subtypes under a single umbrella: Autism Spectrum Disorder (ASD). This marked a shift toward a spectrum model, acknowledging the wide range of experiences and support needs. In the process, previous categories like Asperger’s and PDD-NOS were removed — leading to mixed responses from those who identified with those terms.
- A quiet but significant update: the DSM-5 also allowed clinicians to diagnose autism and ADHD together. Before 2013, they were told to pick one — meaning many of us (especially those with more internalized traits) were diagnosed with ADHD while our autistic traits went unnoticed.
These evolving definitions didn’t change who was Autistic. But they did change who got seen. And for many of us, that shift opened the door to long-overdue recognition.
#2: More Screening = More Identification
In 2007, the American Academy of Pediatrics (AAP) recommended universal autism screening during well-child visits at 18 and 24 months. This policy shift significantly increased early identification, especially among families with access to healthcare.
But that’s just one piece of a larger pattern. Other social and structural changes have also driven up diagnosis rates:
- Greater access to developmental evaluations and pediatric specialists
- School systems increasingly requiring formal diagnoses for IEPs and support services
- A growing “diagnosis-for-access” dynamic, where families pursue identification in order to secure educational accommodations
- Increased awareness among parents, educators, and pediatricians
Public campaigns and cultural shifts, including the United Nations designating April 2nd as World Autism Awareness Day in 2007, and the Autism Self-Advocacy Network reframing it as Autism Acceptance Month in 2011
As awareness grew, so did identification. So understandably we see a sharp increase in numbers:
- In 2000, the CDC reported 1 in 150 children as Autistic
- By 2016, it rose to 1 in 54
- In 2020, it reached 1 in 36
This isn’t over-diagnosis. It’s improved detection. It’s more people being seen, named, and — ideally — supported.
At the same time, access is still far from equal. Disparities in who gets screened, referred, and believed remain a major barrier — especially for BIPOC families and those in under-resourced communities.
But the rise in numbers reflects something bigger than just policy shifts or pediatric screenings. It reflects a cultural shift — a slow but growing ability to recognize autism when it shows up.
#3: We’re Getting Better at Recognizing Underrepresented Groups
Early autism research focused heavily on white, cisgender boys. That narrow prototype shaped decades of clinical assumptions and public awareness.
Now, we’re slowly expanding the frame. Today’s diagnostic practices are better at recognizing autism in:
- Girls and women
- BIPOC individuals
- Genderqueer folx
- Verbally fluent or high-IQ individuals
- Those with co-occurring ADHD, OCD, trauma, or eating disorders
These groups were always autistic. We just didn’t know how to see them.
Research shows that girls often need more pronounced behavioral challenges or intellectual delays to be diagnosed. Many are identified later than boys — if at all — and are frequently misdiagnosed with anxiety or depression first.
Similarly, BIPOC children are less likely to be referred for autism evaluations, require more medical visits to be identified, and are more often given behavioral or conduct-related labels instead.
I explore these disparities more in my infographics on BIPOC, trans, and female autism experiences, as well as in my video series on Substack for Autism Awareness Month.
#4: The Internet Changed Everything
The internet gave Autistic people what traditional institutions didn’t: mirrors.
For decades, most of us only saw autism represented through clinical checklists, deficit-based language, or outdated stereotypes. But then came blogs. Forums. Tumblr. YouTube. TikTok. Online communities where Autistic people — many of us undiagnosed — began sharing our inner worlds in our own words.
And suddenly, we started recognizing ourselves in each other’s stories.
Not in diagnostic manuals, but in posts about sensory overload. Scripts for navigating social fatigue. Photos of stim toys and weighted blankets. Poetic reflections about being “too much” and “not enough” at the same time. It was in these corners of the internet that many of us felt something click:
Wait … that sounds like me.
For some, that self-recognition became a path toward formal diagnosis. For others, it led to self-identification — especially when barriers like cost, race, gender bias, or geography made formal assessment inaccessible. Either way, it offered language, community, and a way to re-narrate our pasts with compassion.
This wasn’t just an increase in numbers. It was the rise of a culture.
Autistic people began finding one another, creating shared rituals and vocabulary, coining terms like “masking” and “neurodivergent,” and building spaces that prioritized sensory safety and authentic expression. We weren’t just identifying ourselves — we were creating belonging.
So when people look at the data and ask, “Why are more people identifying as Autistic now?” — this too is a big part of the answer.
Because we found each other.
Because we saw ourselves.
Because someone else said it out loud, and suddenly… we weren’t alone.
And from that recognition came something more: belonging.
A sense of us.
Not just diagnosis, but community.
Not just traits, but culture.
This wasn’t just awareness — it was awakening.
And it didn’t come from institutions.
It came from us.
#5: Autistic People Grow Up and Fall in Love - And Have Kids
Here’s a less-discussed reason for rising numbers: we pass our traits on… by having sex. We grow up, form relationships, and have children. Sometimes with one another.
Autism is heritable — not in a single-gene way, but through clusters of traits like sensory sensitivity, deep focus, and unique social rhythms. These patterns often run in families — sometimes subtly, sometimes unmistakably.
As more adults recognize their own autism — often prompted by their child’s evaluation — they begin to spot the echoes in themselves, their siblings, their parents. That kind of intergenerational recognition is one reason the numbers are rising.
And there’s more: The rise of online communities and dating apps has made it easier for neurodivergent people to find each other. Shared sensory needs, communication styles, or niche interests can create the foundation for deep, resonant relationships. Research even suggests that Autistic-Autistic pairings may experience higher levels of mutual understanding and rapport than mixed neurotype couples.
So yes, Autistic people are meeting each other online … and sometimes having babies. And maybe — just maybe — that’s contributing to a small, actual rise in prevalence. Not because autism is spreading, but because we’re connecting.
When we see more autistic kids, it’s not an epidemic. It’s an echo. A reflection of Autistic adults finding each other, building families, and continuing a neurodivergent lineage that’s always been here — just hidden.
So... Is there Really an Autism Epidemic?
No. There’s no epidemic. There’s a long-overdue shift in recognition.
Autism isn’t new. What’s new is how we talk about it. How we see it. Who gets seen.
Yes, we’ve watched the numbers climb — from 1 in 150 in the year 2000 to 1 in 36 today. That kind of statistical change can look alarming at first glance. But when we zoom out, we see something more grounded and hopeful:
- We’ve broadened the diagnostic criteria.
- We’ve improved screening and early identification.
- We’re beginning to recognize those who were historically left out.
- We’ve built community and language online, helping people name lifelong experiences.
- And many of us are raising neurodivergent children — not because autism is “spreading,” but because we exist, we connect, and sometimes … we pass our traits on.
So when people ask, “Why are there so many Autistic kids now?”
The answer, in part, is simple:
Because we exist.
Because we find each other.
Because we have kids.
Because we’re no longer invisible.
Could there be a small rise in true prevalence due to environmental or epigenetic factors? Possibly. We can’t completely rule that out. But the overwhelming evidence points to social, clinical, and cultural shifts as the primary drivers behind the rise in diagnoses.
So instead of sounding the alarm, what if we made space?
Space for more accurate narratives.
Space for nuance.
Space for Autistic people to show up fully — in all our diversity, our complexity, our humanness.
The numbers don’t signal a crisis. They reflect a collective awakening..
A long-silenced story finally being told — in full color and full volume.
And maybe, if we keep listening, that story can become a path toward understanding, equity, and care.
Interested In Learning More?
Explore our new course on The Lost Generation of Autistic Adults.
While it’s designed for clinicians, many late-identified adults have found it insightful for their own journey.

Follow-Up Resources
Stay in the Neurodivergent Loop
For ongoing insights and updates, subscribe to the Neurodivergent Insights Newsletter. Each Sunday, I send out fresh thoughts and a roundup of the newest resources on topics related to neurodivergence, mental health, and wellness. My most personal writing is reserved for my newsletter, and subscribers also get access to the newsletter vault (12+ PDFs) when they join.
More like This...



References
About. (n.d.). CDLI. Retrieved January 14, 2025, from https://cdli.mpiwg-berlin.mpg.de/about
https://neurolaunch.com/autism-in-ancient-history/
Autism in the DSM, 1952-2013. (n.d.). Uoregon.edu. Retrieved October 18, 2024, from
Barnard-Brak, L., Richman, D., & Almekdash, M. H. (2019). How many girls are we missing in ASD? An examination from a clinic-and community-based sample. Advances in Autism, 5(3), 214-224.
CDC. (2024, July 19). Data and statistics on autism spectrum disorder. Autism Spectrum Disorder (ASD). https://www.cdc.gov/autism/data-research/index.html
Constantino, J. N., Abbacchi, A. M., Saulnier, C., et al. (2020). Timing of the diagnosis of autism in African American children. Pediatrics, 146(e20193629).
Crompton, C. J., Ropar, D., Evans-Williams, C. V., Flynn, E. G., & Fletcher-Watson, S. (2020). Autistic peer-to-peer information transfer is highly effective. Autism : the international journal of research and practice, 24(7), 1704–1712.
Crompton, C. J., Sharp, M., Axbey, H., Fletcher-Watson, S., Flynn, E. G., & Ropar, D. (2020). Neurotype-Matching but Not Being Autistic Influences Self and Observer Ratings of Interpersonal Rapport. Frontiers in Psychology, 11, 586171.
Donvan, J., & Zucker, C. (2016, January 6). The early history of autism in America. Smithsonian Magazine.
Dworzynski, K., Ronald, A., Bolton, P., & Happé, F. (2012). How Different Are Girls and Boys Above and Below the Diagnostic Threshold for Autism Spectrum Disorders? Journal of the American Academy of Child and Adolescent Psychiatry, 51(8), 788–797.
Durkin, M. S., Maenner, M. J., Baio, J., et al. (2017). Autism spectrum disorder among US children (2002–2010): Socioeconomic, racial, and ethnic disparities. American Journal of Public Health, 107(11), 1818–1826.
Milton, D. E. M. (2012). On the ontological status of autism: the ‘double empathy problem.’ Disability & Society, 27(6), 883–887.
Happé, F., & Frith, U. (2020). Annual Research Review: Looking back to look forward – changes in the concept of autism and implications for future research. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 61(3), 218–232.
Humphrey, N. (1998). Cave art, autism, and the evolution of the human mind. Cambridge Archaeological Journal, 8(2), 165–191.
Kanner, L. (1949). Problems of nosology and psychodynamics of early infantile autism. The American Journal of Orthopsychiatry, 19(3), 416–426.
Kanner, Leo, & Lesser, L. I. (1958). Early infantile autism. Pediatric Clinics of North America, 5(3), 711–730.
Johnson CP, Myers SM; American Academy of Pediatrics Council on Children With Disabilities . Identification and evaluation of children with autism spectrum disorders. Pediatrics. 2007;120(5):1183–1215
Mandell, D. S., Ittenbach, R. F., Levy, S. E., et al. (2007). Disparities in diagnoses received prior to a diagnosis of autism spectrum disorder. Journal of Autism and Developmental Disorders, 37, 1795–1802.
Spikins, P., Scott, C., & Wright, B. (2018). How do we explain ‛autistic traits’ in European Upper Palaeolithic art? Open Archaeology, 4(1), 262–279.
Waltz, M., & Shattock, P. (2004). Autistic disorder in nineteenth-century London: three case reports: Three case reports. Autism: The International Journal of Research and Practice, 8(1), 7–20.
Wiggins, L. D., Durkin, M., Esler, A., Lee, L. C., Zahorodny, W., Rice, C., Yeargin-Allsopp, M., Dowling, N. F., Hall-Lande, J., Morrier, M. J., Christensen, D., Shenouda, J., & Baio, J. (2020). Disparities in Documented Diagnoses of Autism Spectrum Disorder Based on Demographic, Individual, and Service Factors. Autism research : official journal of the International Society for Autism Research, 13(3), 464–473.
Rivet, T.T. and Matson, J.L. (2011), “Review of gender differences in core symptomatology in autism spectrum disorders”, Research in Autism Spectrum Disorders, Vol. 5 No. 3, pp. 957-76.
Sher, D. A., & Gibson, J. L. (2023). Pioneering, prodigious and perspicacious: Grunya Efimovna Sukhareva’s life and contribution to conceptualising autism and schizophrenia. European Child & Adolescent Psychiatry, 32(3), 475–490.
Previous Graphics