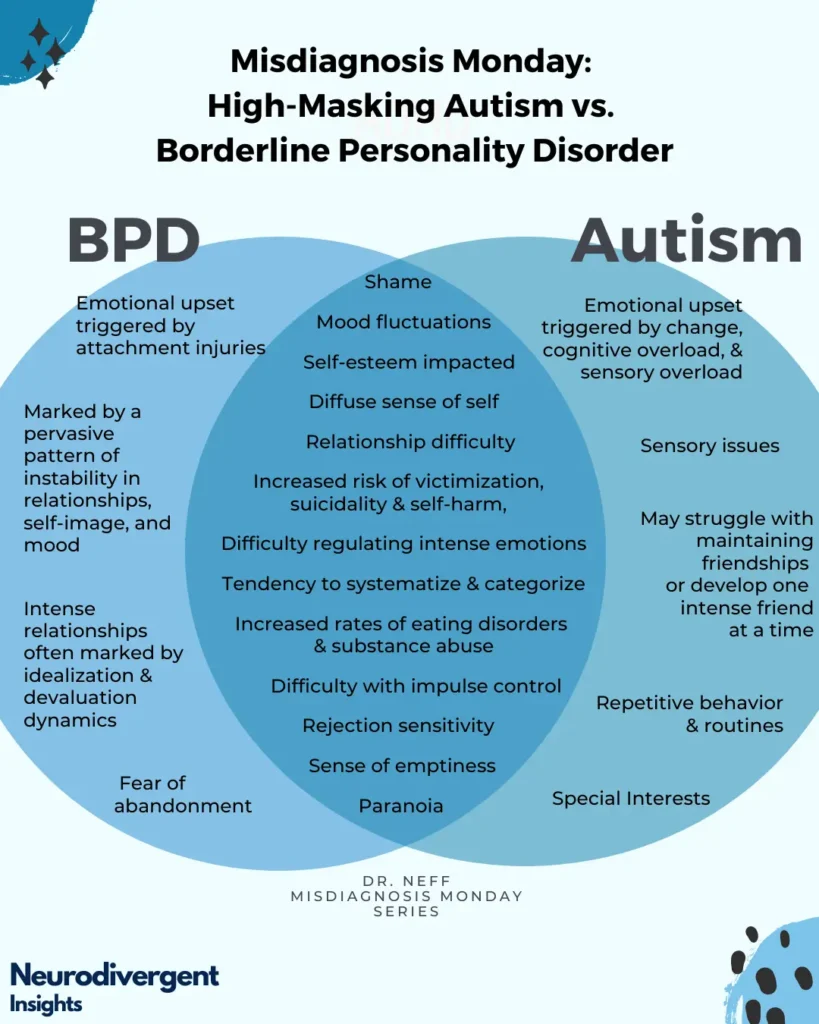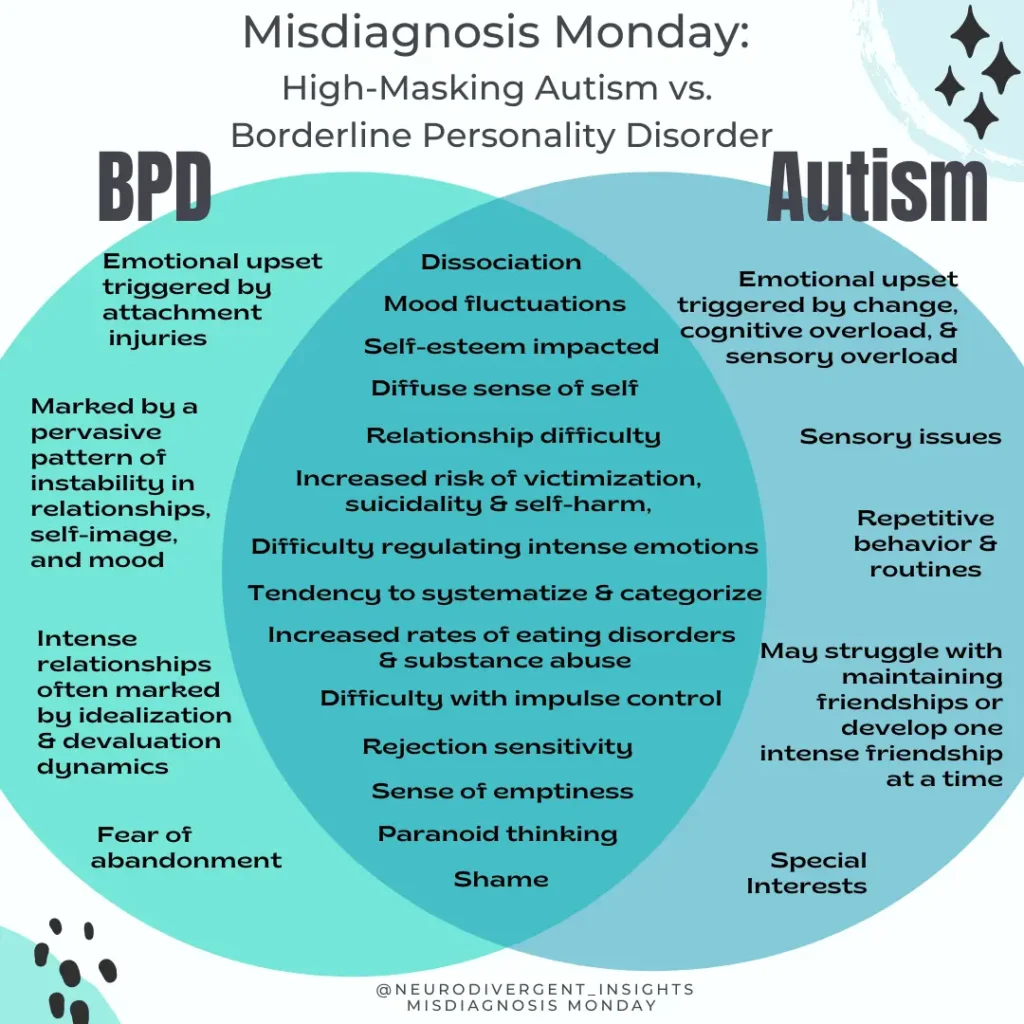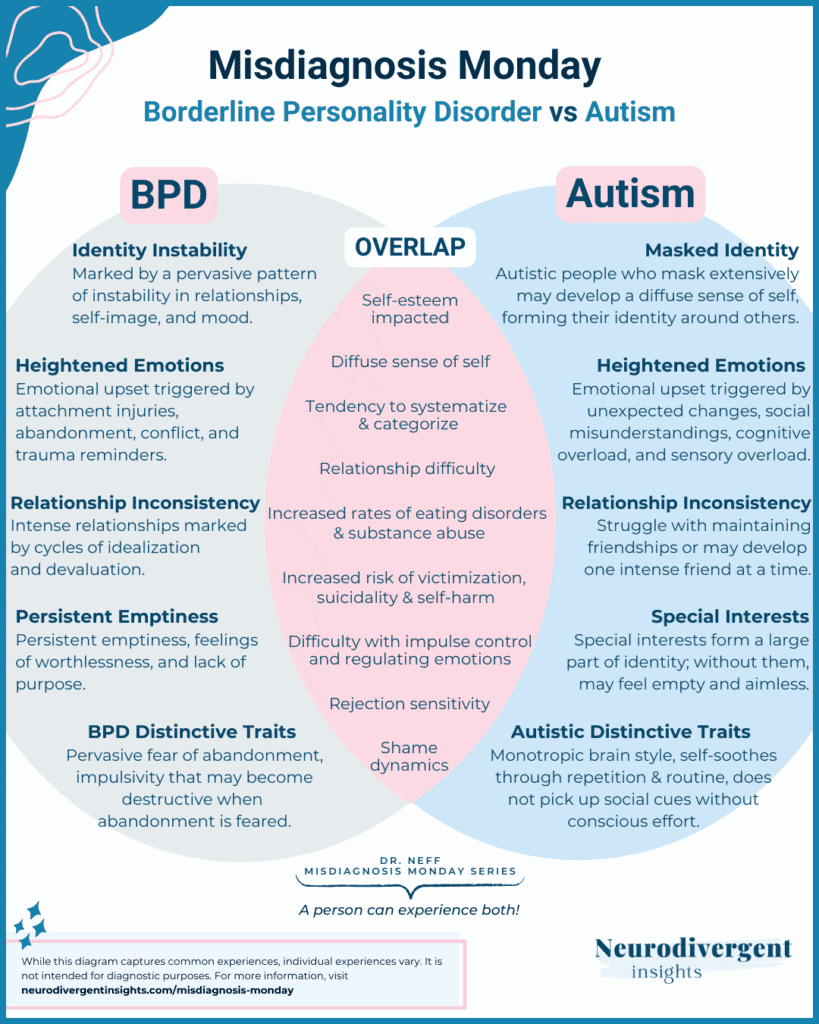
Borderline Personality Disorder vs. Autism
Borderline Personality Disorder is a common misdiagnosis for Autistic women and genderqueer people. Complicating matters, BPD and Autism also co-occur at high rates, and an Autistic person is more vulnerable to developing BPD. So a person may have both Autism and BPD. When the underlying Autism is missed, BPD symptoms are likely exacerbated.
Unfortunately, many clinicians are not considering Autism when assessing for BPD. It is important Autism is always ruled-out or on the differential list when assessing for BPD. This is particularly important given that an Autistic neurotype makes a person more vulnerable to developing BPD.
This article offers a brief description of their many overlapping traits and experiences.
Table of Contents
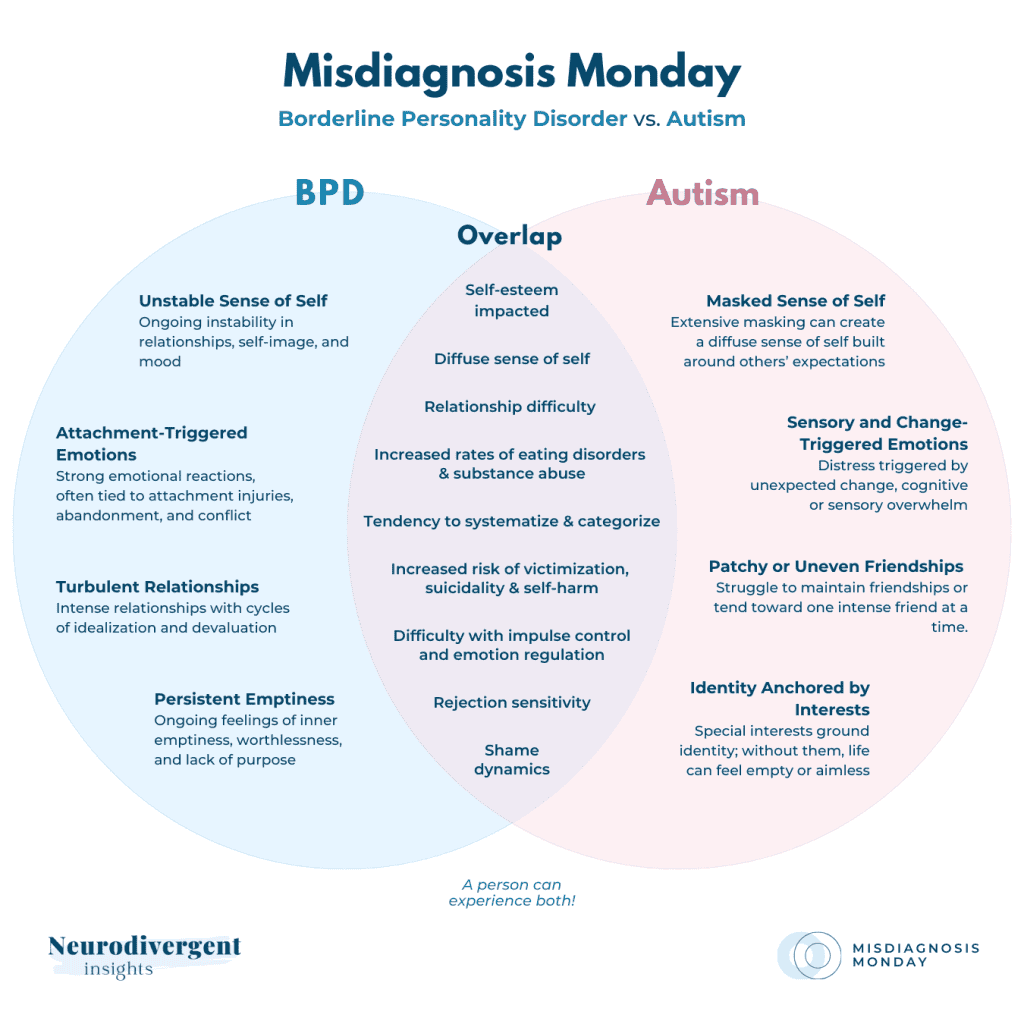
Overlapping Autistic and BPD Traits
Sensitivity to Abandonment
Rejection Sensitive Dysphoria is common among Autists and ADHDers. Rejection sensitivity is an intense sensitivity to rejection or perceived rejection. People with RSD often go to great lengths to avoid situations that cause them to feel rejected. They also have strong reactions when they perceive themselves as being rejected.
For more information about Rejection Sensitive Dysphoria and how to cope, check out the full workbook here.
A Diffuse Sense of Self
A diffuse sense of self. A core feature of BPD is a “diffuse sense of self” or lack of “self-identity,” often resulting from early childhood development/trauma. High-masking autists, who learn to socialize through copying/becoming chameleons, often lack a true social identity (Attwood, Vid.1).
Chronic Feelings of Emptiness
These feelings are commonly reported among high-masking autistics. This likely is related to diffuse identity due to social masking. Many autists also experience a sense of emptiness during burnout and when not actively engaged in a task (Attwood vid.2).
Social Difficulties
Social interactions & maintaining long-term relationships can be challenging for both groups. However, the core reasons behind difficulty often have different origins and must be considered.
Emotional Dysregulation
Emotional dysregulation is a core feature of BPD. Autists also struggle with emotional dysregulation due to the autistic brain wiring/chemistry. Sensory overload and sensory meltdowns can also lead to emotional dysregulation.
Relationship Difficulty
Relationships can be challenging for both groups. This is due to differences in social cognition, social interactions, and maintaining long-term.
Sexual and Gender Diversity and Fluidity
Gender-queering is more common among Autistic people and people with BPD. People with BPD more commonly shift in their core sense of self, including sexual and gender identity (Biskin and Paris).
Autistic people are more likely than NTs to be gender diverse, and gender-diverse people are more likely to have autism than cisgender people.
People who don’t identify with the sex they were assigned at birth are 3-6 times more likely to be Autistic than cisgender people (Warrier et al.)
Autistics are more likely to be non-heterosexual than the general population (Sarris).
Emerging research demonstrates a higher percentage of gay and gender-diverse individuals represented within BPD populations (Reuter et al. and Singh).
Depersonalization and Derealization
Depersonalization involves the sensation that a person’s body/self is unreal or altered in a strange way.
Derealization involves the experience of the external world being bizarre, unreal, or dream-like.
Both can be a response to trauma; however, they can also be a response to sensory overload as the body shuts down to keep from taking in more sensory information. These experiences are common among both groups (Botbol).
Insecure Attachment Style
BPD is characterized by an insecure attachment style (typically anxious/preoccupied) (Agrawal et al.).
Autistic people often experience insecure attachments. Autistic people are more likely to have an avoidant attachment style: One study found a higher rate of avoidant attachment styles among Autistic individuals. No association was found between anxious attachment and autistic traits) (McKenzie and Dallos).
Another study found Autistic children had higher rates of disorganized attachment (22%). Certain Autistic behaviors may look like a disorganized attachment. Thus, it can be challenging to identify an autistic trait vs. a disorganized attachment style (Coughlan et al.).
Overlapping Risks
Eating Disorders
Both have a high % of eating disorders (may function as a method of self-soothing/gaining a sense of control)
One study found that 53.8% of people with BPD met the criteria for an Eating Disorder (21.7% anorexia nervosa and 24.1% bulimia nervosa) (Salters-Pedneault).
While the rates vary, most researchers agree that about 23% of people diagnosed with anorexia nervosa are Autistic. However, it is likely an underrepresentation due to the fact Autism often goes undiagnosed within this population (Westwood and Tchanturia).
Substance Abuse/Addiction
Substance abuse/addiction: For a long time, it was assumed that substance abuse was low among autists (due to adherence to rules).
Emerging research shows the hidden side of autistic addiction. A recent study in Sweden found that Autistic people with average to high intelligent quotients (IQ) were twice as likely to struggle with addiction to alcohol or other drugs. Among Autists, drugs are sometimes used to cope with social stress and sensory problems (Szalavitz).
Alcohol and drugs are a powerful way of attempting to regulate one’s nervous system when it is flooded with stress hormones. This can be a common way a person self-soothes following trauma. Approximately half of the people with BPD also have a co-occurring substance abuse disorder, often alcohol (Trull et al.).
Victimization
Victimization: Both groups have elevated risks of victimization (Botbol). Recent research has demonstrated that Autistic women and genderqueer people are more likely to be survivors of violent victimization. Some risk factors include:
challenges in social reasoning
missing contextual cues
a tendency to take things literally
One study found that Autistic adults were 7.3 times more likely to endorse past experiences of sexual assault (Weiss and Fardella).
Suicidality
Autists with average to high IQ are three times more likely to attempt or die by suicide than the general population (South et al.)
Self-Harm
Self-harm is common among both groups. Self-harm more commonly happens in the context of sensory overload for Autists. In the context of BPD, it more often occurs following an attachment injury (Botbol).
One study found that parents reported self-harm behavior among their autistic youth in 15% of cases (Huang).
Autistic teenagers are also more likely to engage in self-harm behavior. Self-harm can be in the form of cutting, skin-picking, hair-pulling, and hitting.
Eating Disorders
Both Groups have a high percentage of eating disorders. One study found that 53.8% of people with BPD met the criteria for an Eating Disorder (21.7% anorexia nervosa and 24.1% bulimia nervosa) (Salters-Pedneault).
While the rates vary, most researchers agree that about 23% of people diagnosed with anorexia nervosa are Autistic. However, many agree this is likely an underrepresentation due to the fact Autism often goes undiagnosed within this population (Westwood and Tchanturia)
Co-occurring Mood Disorders
Both groups have an elevated risk of having co-occurring mood disorders such as depression and anxiety.
According to one study, 79% of Autists met the criteria for a co-occurring psychiatric tradition at least once in their life (Lever and Geurts).
Major depressive disorder and PTSD commonly co-occur with BPD. One study reported 83% of those with BPD would meet the criteria for Major Depression at least once in their life (Beatson).

Summary
Autism and Borderline Personality can both co-occur, or they can be misdiagnosed as one another. To the untrained eye, undiagnosed autism can easily look like BPD. To understand the difference, it is important to 1) Consider the possibility of autism and 2) Understand the internal experience of the person to tease out autism traits from BPD symptoms. For more of a deep dive into the similarities and differences, check out the full workbook here.
Follow-Up Resources
Stay in the Neurodivergent Loop
For ongoing insights and updates, subscribe to the Neurodivergent Insights Newsletter. Each Sunday, I send out fresh thoughts and a roundup of the newest resources on topics related to neurodivergence, mental health, and wellness. My most personal writing is reserved for my newsletter, and subscribers also get access to the newsletter vault (12+ PDFs) when they join.
More Like This...
Previous Graphics