Updated April 1st, 2026

The first memory I have of depression is from when I was five or six. I remember crawling into my closet, pulling my knees tight to my chest, and feeling like there was a dark wall between me and the rest of the world.
When the waves would hit, that’s how I described it to my mom: it felt like being locked away behind that wall. I ebbed in and out of depression throughout childhood and my teen years, and it still shows up as an unwelcome companion at times in my adult life. As an ADHDer, that doesn’t make me an exception; it places me squarely inside the ADHD norm.
As an ADHDer and a clinical psychologist, I’ve sat on both sides of this. I’ve been the clinician trying to sort out whether someone’s low mood is depression, ADHD burnout, or the long tail of a missed ADHD diagnosis. And I’ve been the person lying awake at night wondering why I can’t seem to care about anything, even things I usually love.
ADHDers are significantly more likely to experience depression than the general population, but it’s not a simple “ADHD causes depression” story. It’s about what it means to live in an ADHD body and nervous system while navigating systems that are often misaligned with our way of being.
In this article, I’ll walk through how common ADHD + depression really is, why they’re so tangled, what emotional dysregulation and rejection sensitivity have to do with it, how to tell ADHD burnout from depression, and what kinds of support actually help.
Table of Contents
How common is co‑occurring ADHD and depression?
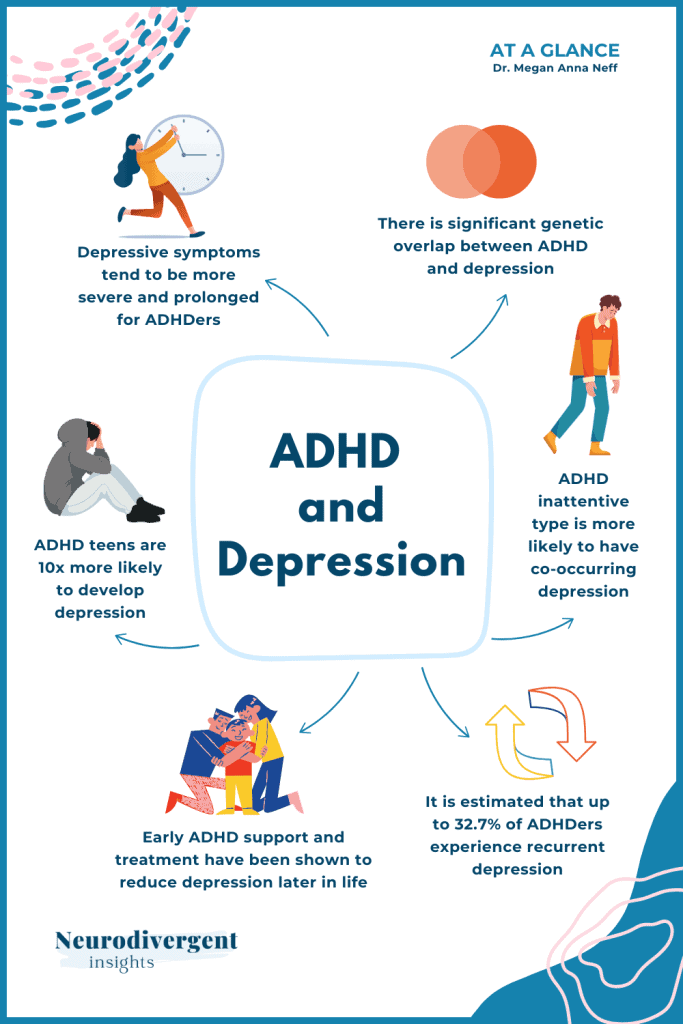
Different studies give different exact numbers, but they tell a very similar story: ADHDers carry a much higher depression risk across the lifespan.
When researchers pooled dozens of studies in a 2025 meta‑analysis, they found that children and teens with ADHD were more than twice as likely to develop depression as their non‑ADHD peers. That pattern doesn’t disappear in adulthood. Large reviews of adult ADHD consistently find that a substantial portion of ADHDers will experience a depressive episode, and many will receive a formal depression diagnosis at some point in their lives.
A large Swedish population study went even further, following over a million people and comparing those with ADHD to their non‑ADHD siblings. Even after accounting for shared family factors, the ADHD group still had markedly higher rates of depression, suggesting that ADHD itself, not just shared genes or environment, is part of the story.
Long‑term follow‑up studies of children diagnosed with ADHD in early childhood have found that they are several times more likely to develop depression in the years that follow compared to non‑ADHD peers.
Clinically and personally, what stands out to me is that the risk doesn’t “burn off” with age. For many ADHDers, depression doesn’t show up clearly until adulthood, perhaps after years of compensating, masking, overworking, and living without language for all they are navigating.
Why are ADHD and depression so connected?
There are several overlapping pathways. Most ADHDers I work with have multiple of these running at once.
Shared genetic terrain
ADHD is one of the most heritable conditions we see in mental health, and depression also has a strong genetic component. Newer genetic studies suggest a meaningful overlap between the sets of genes that raise likelihood for ADHD and those that raise risk for major depression.
You can think of it as shared biological “soil”: the same ground can grow different plants. Having this shared terrain doesn’t mean depression is inevitable if you have ADHD, but it helps explain why they are so frequently found together.
There is also early molecular research hinting that some of the proteins involved in ADHD are tied to depression biology as well. I hold this lightly: it is interesting and validating, but it does not change the day‑to‑day reality that we still need practical supports and environments that fit.
Emotional dysregulation: a key bridge
Emotional dysregulation is increasingly recognized as a core feature of ADHD, not just a side effect. Many ADHDers describe emotions that arrive quickly, feel very intense, and take a long time to settle — a nervous system that doesn’t have easy “dimmer switches” for emotional states.
In one 2025 longitudinal study of young people with ADHD, researchers asked what actually carries some kids from ADHD into depression as they get older. They found that emotion regulation was a key bridge. Two patterns were especially important:
- A tendency to catastrophize — assuming the worst is about to happen.
- Difficulty shifting attention away from distressing thoughts or sensations once they’ve been activated.
Hyperactive‑impulsive traits in childhood tended to connect to later depression more through catastrophizing, while inattentive traits connected more through difficulty disengaging from negative thoughts. For many ADHDers, this will feel familiar: the impulsive brain doesn’t just act without thinking; it has a hard time pivoting away from painful or loud thoughts and emotions.
Over time, repeated cycles of emotional overwhelm plus limited tools or support can erode mood and self‑trust. It is very hard to feel hopeful when your nervous system regularly hijacks you, and the people around you interpret that as “overreacting” or “being dramatic.”
Rejection sensitivity and the quiet slide into withdrawal
Many ADHDers experience intense emotional pain in response to perceived criticism, disapproval, or rejection. This is often called rejection sensitive dysphoria (RSD), though the formal research uses slightly different language.
A qualitative study of ADHDers published in 2026 described rejection sensitivity as setting off a chain reaction:
emotional pain → masking and people‑pleasing → self‑alienation → withdrawal and loneliness → depression.
In other words, it’s not just the sting of rejection itself; it’s the way people contort themselves afterward, and the isolation that follows.
The ADHD nervous system registers social threat very strongly and very quickly. When the nervous system’s solution is to hide, shut down, or avoid connection altogether, it creates the perfect context for depression to grow.
I explore this more in my pieces on rejection sensitive dysphoria and on how RSD plays out in friendships, where these relational loops show up in day‑to‑day life.
The accumulated weight of the ADHD experience
Then there is the slow, grinding impact of living with ADHD, especially when it’s unrecognized or unsupported.
Research and lived experience both point to elevated rates of:
- Social rejection and peer difficulties in childhood.
- Critical feedback from adults who misinterpret ADHD traits as laziness, carelessness, or defiance.
- Academic and work underachievement compared to underlying ability.
A 2023 review focusing on women with ADHD found that they are more likely to be diagnosed with depression or anxiety before anyone screens for ADHD, and more likely to be offered antidepressants before ADHD medications. When the ADHD piece is missed, treatment centers on mood alone, and the daily ADHD friction keeps generating new reasons to feel hopeless or “broken.”
For gender diverse ADHDers, the picture is even more complex, with higher rates of misdiagnosis, minority stress, and invalidation, all of which increase depression risk.
Risk Factors of Co-occurrence
Not every ADHDer will experience depression, but some patterns do raise the likelihood:
Late or missed ADHD diagnosis. When ADHD goes unrecognized for years, people are left to “white‑knuckle” life with no language or support for what is happening. A large 2025 review found that children and teens who received stimulant treatment had a lower risk of developing depression over time, which suggests that treating ADHD early may protect mood for some people.
Being female or gender diverse. Women and gender diverse ADHDers are more likely to be diagnosed with anxiety or depression first, and only later does anyone think to screen for ADHD. Hormonal shifts across the menstrual cycle, pregnancy, perimenopause, and beyond can also amplify both ADHD symptoms and mood vulnerability, increasing the risk of depression during already tender seasons.
- Inattentive‑leaning ADHD. Inattentive ADHD is more strongly linked with internalizing conditions like depression. This same presentation is also more likely to be missed, particularly in quiet, high‑masking ADHDers. Being praised for being “no trouble” while struggling internally is a setup for self‑blame.
- Co‑occurring conditions and chronic stress. Anxiety, trauma, oppositional patterns, and chronic physical health issues all add load to a nervous system that’s already working hard. Without more support, that extra load often shows up as depression.
- High emotional dysregulation. ADHDers who catastrophize, ruminate, or get stuck in emotional states—especially in invalidating environments—are at particular risk, because the path from emotional overwhelm to low mood is shorter and steeper.
Is it ADHD Burnout or Depression?
This is one of the questions I hear most often from ADHDers: “Is this depression, or is this ADHD burnout?” The answer is often “some of both,” but it’s worth teasing apart.
From the outside, ADHD burnout and depression can look almost identical:
- Exhaustion and low energy.
- Withdrawing and pulling away from social activities.
- Difficulty starting and finishing tasks.
- Losing interest in things that used to matter.
But there are important differences in how they work under the surface.
What ADHD burnout is
ADHD burnout is usually driven by chronic overextension: years of masking, sustained compensatory effort, sensory overload, and running your life in environments that don’t fit your ADHD nervous system. It often includes:
- Pervasive exhaustion that doesn’t fully resolve with a single weekend of rest.
- Heightened sensory sensitivities and “sensory sickness.”
- A drop in executive functioning and daily living skills (e.g., basic chores feel impossible).
Autistic burnout research has described this combination as “having all your internal resources exhausted beyond measure and being left with no clean‑up crew,” and many ADHDers resonate with this description as well.
In ADHD burnout, the primary problem is overload and mismatch between demands and capacity, not necessarily a core mood disorder— though mood absolutely suffers.
What depression is
Clinical depression centers on mood changes and shifts in how we view ourselves and the world. Common features include:
- Persistent low mood or irritability.
- Anhedonia, or loss of pleasure or interest.
- Feelings of worthlessness, guilt, or hopelessness.
- More pronounced changes in sleep and appetite patterns.
Depression can show up in ADHDers with or without burnout. It can be triggered by life events, trauma, chronic stress, or seemingly “out of the blue,” likely drawing on those genetic and biological vulnerabilities we talked about earlier.
Why the distinction matters
Standard depression treatments often involve behavioral activation: gently increasing meaningful activities to counter withdrawal and passivity. When someone is in ADHD or autistic burnout, though, pushing more activity without reducing demands can make things worse.
In burnout, what is often most healing is:
- Reducing demands where possible.
- Increasing rest and sensory recovery.
- Dropping non‑essential obligations.
- Unmasking in safe contexts.
- Adjusting environments to fit the actual nervous system.
When depression is present alongside burnout (which is very common), we usually need a both/and approach: tending to depletion and nervous system overload and addressing mood, thoughts, and relational wounds. That’s a different path than treating depression alone.
What co‑occurring ADHD and depression means for daily life
When ADHD and depression show up together, they tend to make each other heavier.
Depression tends to deepen the core ADHD struggles with initiation, planning, and follow‑through. Tasks that already required extra effort now feel impossible. The familiar “I know what I should do but can’t make myself do it” of ADHD becomes heavier when depression takes away what little fuel was left.
Research echoes this: adults with both ADHD and depression tend to:
- have more severe and longer‑lasting depressive episodes
- higher suicidal risk, and
- greater overall healthcare use than those with ADHD alone
One recent study recent study even found that healthcare costs were roughly doubled in adults with both ADHD and depression, mirroring how it often feels internally: more appointments, more crises, more energy spent explaining yourself.
Subjectively, many ADHDers describe this combination as living with a brain that already needs more scaffolding and margin, at the same time as depression erodes motivation, hope, and self‑compassion. It can feel like trying to run a marathon with a sprained ankle while been told is “just in your head.”
Approaches to support and treatment
There is no single right sequence for treating co‑occurring ADHD and depression, but there are some helpful principles.
Addressing the ADHD
Current clinical guidelines tend to recommend starting with whichever condition is most impairing, while not ignoring the other. For many ADHDers, supporting ADHD, through medication, environmental modifications, or both, indirectly lifts mood by reducing the ongoing friction that feeds hopelessness and self‑criticism.
Large population‑level studies from Sweden and elsewhere suggest that stimulant medications are linked with fewer psychiatric hospitalizations and lower rates of suicidal behavior in people with ADHD. The same 2025 meta‑analysis I mentioned earlier also found that stimulant treatment was associated with a modest reduction in depression risk over time.
Medication is not accessible or appropriate for everyone, but leaving ADHD untreated or under‑treated is, in itself, a depression risk factor.
Environmental supports also matter: flexible work arrangements, sensory‑friendly spaces, realistic expectations around productivity, and tools for executive functioning can all lighten the load on an ADHD nervous system.
Therapy that understands both ADHD and depression (and burnout)
Therapy can be genuinely helpful here, but it needs to be ADHD‑literate and burnout‑aware.
An ADHD‑informed therapist will:
- Differentiate between “avoidance” driven by depression and “adaptive withdrawal” needed for burnout recovery.
- Adapt behavioral activation so it doesn’t simply add more demands to an already maxed‑out system.
- Recognize that not every “negative thought” is a distortion; some accurately reflect ableist systems or unsupported environments.
- Support you in integrating a positive neurodivergent-identity which can help in reducing shame or feelings of inadequacy.
Approaches that directly target emotional dysregulation, such as dialectical behavior therapy (DBT) skills, acceptance and commitment therapy (ACT), or trauma‑informed emotion regulation work, can be particularly useful in addressing that ADHD‑to‑depression bridge.
Nervous system care
Because emotional dysregulation and chronic hyper‑ or hypo‑arousal are so central, nervous system care is not “extra”; it is core depression prevention for ADHDers.
This can include:
- Sensory regulation (identifying and meeting your sensory needs on purpose).
- Movement that feels regulating rather than punishing.
- Building in more true rest and fewer cheap dopamine “hits” that leave you more drained.
- Completing the stress cycle regularly rather than staying in chronic activation.
If you’re looking for more guided resources on nervous system resets and sensory regulation that offer concrete tools for this work you can check out the Nervous System and Sensory Workbook.
Community and connection
Isolation is both a symptom of depression and a risk factor for it. For ADHDers, being in spaces with other neurodivergent people can soften the sense of being uniquely broken. Many readers tell me that hearing other ADHDers describe the same “weird” patterns and ways of being have been protective against depression.
At the same time, it is important to name that “just reach out” is not simple when you are depressed or burned out. Low‑demand connection through things like parallel play, text‑based contact, being with someone without needing to perform, often fits better at these times than high‑energy socializing.
Summary
For many ADHDers, depression is not an isolated diagnosis that appeared next to ADHD on a chart. It is woven into years of being unaccommodated in systems that reward consistency, predictability, and narrow bands of emotional expression.
Understanding the links between ADHD and depression doesn’t make the depression vanish. It can, however, gently shift the story from “something is wrong with me” to “my nervous system and my environments have been in a long mismatch, and my system is showing the strain.”
For a lot of people, that shift is the first small opening toward different kinds of support, different expectations, and, eventually, a different relationship with both ADHD and mood.
If you want to learn more about depression and neurodivergence and discover strategies for breaking the cycle of depression, you can find my workbook on the topic here.
Follow-Up Resources
The Help Me Stay Plan (Free Resource)

The Help Me Stay Plan is a completely free resource our NDI team created in honor of those we’ve lost to suicide and those who have come close. If you live with depression or suicidal thoughts and feel alone in these experiences, we hope this resource can be one small anchor point for you.
The ADHD Starter Pack
The ADHD Starter Pack includes our three most popular ADHD workbooks to help you get to know your ADHD brain and build ways of working with it, not against it.
Stay in the Neurodivergent Loop
For ongoing insights and updates, subscribe to the Neurodivergent Insights Newsletter. Each Sunday, I send out fresh thoughts and a roundup of the newest resources on topics related to neurodivergence, mental health, and wellness. My most personal writing is reserved for my newsletter, and subscribers also get access to the newsletter vault (12+ PDFs) when they join.
More Like This...



References
Attoe, D. E., & Climie, E. A. (2023). Miss. Diagnosis: A Systematic Review of ADHD in Adult Women. Journal of attention disorders, 27(7), 645–657. https://doi.org/10.1177/10870547231161533
Blackman, G. L., Ostrander, R., & Herman, K. C. (2005). Children with ADHD and depression: a multisource, multimethod assessment of clinical, social, and academic functioning. Journal of attention disorders, 8(4), 195-207.
Bron, T. I., Bijlenga, D., Verduijn, J., Penninx, B. W., Beekman, A. T., & Kooij, J. J. (2016). Prevalence of ADHD symptoms across clinical stages of major depressive disorder. Journal of affective disorders, 197, 29–35.
Chang, Z., D’Onofrio, B. M., Quinn, P. D., Lichtenstein, P., & Larsson, H. (2016). Medication for attention-deficit/hyperactivity disorder and risk for depression: A nationwide longitudinal cohort study. Biological Psychiatry, 80(12), 916–922. PubMed
Chronis-Tuscano, A., Molina, B. S., Pelham, W. E., Applegate, B., Dahlke, A., Overmyer, M., & Lahey, B. B. (2010). Very early predictors of adolescent depression and suicide attempts in children with attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 67(10), 1044–1051.
Daviss, W. B., & Bond, J. B. (2016). Comorbid ADHD and depression: assessment and treatment strategies. Psychiatr Times, 33(9).
de la Peña, I. C., Pan, M. C., Thai, C. G., & Alisso, T. (2020). Attention-Deficit/Hyperactivity Disorder Predominantly Inattentive Subtype/Presentation: Research Progress and Translational Studies. Brain sciences, 10(5), 292. https://doi.org/10.3390/brainsci10050292
Faraone, S. V., & Larsson, H. (2019). Genetics of attention deficit hyperactivity disorder. Molecular psychiatry, 24(4), 562–575.
Fu X, Wu W, Wu Y, Liu X, Liang W, Wu R and Li Y (2025) Adult ADHD and comorbid anxiety and depressive disorders: a review of etiology and treatment. Front. Psychiatry 16:1597559. doi: 10.3389/fpsyt.2025.1597559
Garcia-Argibay M, Brikell I, Thapar A …
Attention-Deficit/Hyperactivity Disorder and Major Depressive Disorder: Evidence From Multiple Genetically Informed Designs
Biological Psychiatry, 2023; 95, 444-452
Goodman, D. W., & Thase, M. E. (2009). Recognizing ADHD in adults with comorbid mood disorders: implications for identification and management. Postgraduate medicine, 121(5), 20–30.
Gundel, L. K., Pedersen, C. B., Munk-Olsen, T., & Dalsgaard, S. (2018). Longitudinal association between mental disorders in childhood and subsequent depression – A nationwide prospective cohort study. Journal of Affective Disorders, 227, 56–64.
Mitchison, G. M., & Njardvik, U. (2019). Prevalence and gender differences of ODD, anxiety, and depression in a sample of children with ADHD. Journal of attention disorders, 23(11), 1339-1345.
Riglin, L., Leppert, B., Dardani, C., Thapar, A., Rice, F., O’Donovan, M., . . . Thapar, A. (2021). ADHD and depression: Investigating a causal explanation. Psychological Medicine, 51(11), 1890-1897. doi:10.1017/S0033291720000665
Rowney-Smith, A., Sutton, B., Quadt, L., & Eccles, J. A. (2026). The lived experience of rejection sensitivity in ADHD – A qualitative exploration. PloS one, 21(1), e0314669. https://doi.org/10.1371/journal.pone.0314669
Schein, J., Cloutier, M., Gauthier-Loiselle, M., Bungay, R., Chen, K., Chan, D., & Childress, A. (2024). Health care resource utilization and costs associated with psychiatric comorbidities in adult patients with attention-deficit/hyperactivity disorder. Journal of managed care & specialty pharmacy, 30(6), 588–598. https://doi.org/10.18553/jmcp.2024.30.6.588
Taipale, H., Bergström, J., Gèmes, K., Tanskanen, A., Ekselius, L., Mittendorfer-Rutz, E., & Helgesson, M. (2024). Attention-Deficit/Hyperactivity Disorder Medications and Work Disability and Mental Health Outcomes. JAMA network open, 7(3), e242859. https://doi.org/10.1001/jamanetworkopen.2024.2859
Tharaud, J. B., & Nikolas, M. A. (2025). Emotion regulation as a transdiagnostic link between ADHD and depression symptoms: evidence from a network analysis of youth in the ABCD study. Child and adolescent psychiatry and mental health, 19(1), 113. https://doi.org/10.1186/s13034-025-00966-6
Zhang, Y., Liao, W., Rao, Y., Gao, W., & Yang, R. (2025). Effects of ADHD and ADHD medications on depression and anxiety in children and adolescents: A systematic review and meta-analysis. Journal of psychiatric research, 181, 623–639. https://doi.org/10.1016/j.jpsychires.2024.12.022
Previous Graphics